Service de Soins Intensifs, Hôpital du Sacré-Coeur de Montréal, CIUSSS du Nord-de l'île de Montréal, Département de Médecine, Université de Montréal, 5400 Gouin Ouest, Montreal, QC, H4J 1C5, Canada.
ERESI (Equipe de Recherche En Soins Intensifs), Centre de recherche de l'Hôpital du Sacré-Coeur de Montréal, Montreal, QC, Canada.
Can J Anaesth. 2021 Feb;68(2):204-213. doi: 10.1007/s12630-020-01816-z. Epub 2020 Sep 15.
Montreal has been the epicentre of the coronavirus disease (COVID-19) pandemic in Canada. Given the regional disparities in incidence and mortality in the general population, we aimed to describe local characteristics, treatments, and outcomes of critically ill COVID-19 patients in Montreal.
A single-centre retrospective cohort of consecutive adult patients admitted to the intensive care unit (ICU) of Hôpital du Sacré-Coeur de Montréal with confirmed COVID-19 were included.
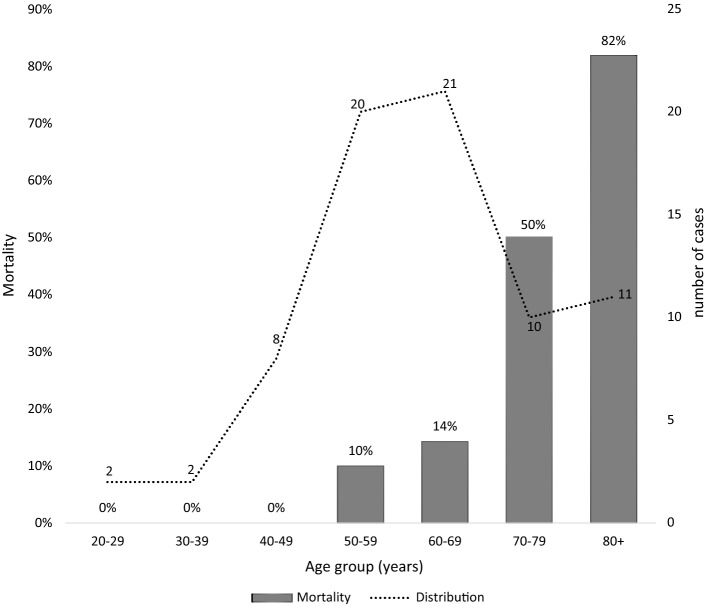
Between 20 March and 13 May 2020, 75 patients were admitted, with a median [interquartile range (IQR)] age of 62 [53-72] yr and high rates of obesity (47%), hypertension (67%), and diabetes (37%). Healthcare-related infections were responsible for 35% of cases. The median [IQR] day 1 sequential organ failure assessment score was 6 [3-7]. Invasive mechanical ventilation (IMV) was used in 57% of patients for a median [IQR] of 11 [5-22] days. Patients receiving IMV were characterized by a moderately decreased median [IQR] partial pressure of oxygen:fraction of inspired oxygen (day 1 PaO:FO = 177 [138-276]; day 10 = 173 [147-227]) and compliance (day 1 = 48 [38-58] mL/cmHO; day 10 = 34 [28-42] mL/cmHO) and very elevated estimated dead space fraction (day 1 = 0.60 [0.53-0.67]; day 10 = 0.72 [0.69-0.79]). Overall hospital mortality was 25%, and 21% in the IMV patients. Mortality was 82% in patients ≥ 80 yr old.
Characteristics and outcomes of critically ill patients with COVID-19 in Montreal were similar to those reported in the existing literature. We found an increased physiologic dead space, supporting the hypothesis that pulmonary vascular injury may be central to COVID-19-induced lung damage.
蒙特利尔是加拿大冠状病毒病(COVID-19)大流行的中心。鉴于普通人群中发病率和死亡率的区域性差异,我们旨在描述 COVID-19 重症患者在蒙特利尔的当地特征、治疗方法和结局。
对 2020 年 3 月 20 日至 5 月 13 日期间入住蒙特利尔 Sacré-Coeur 医院重症监护病房(ICU)的连续确诊 COVID-19 成年患者进行单中心回顾性队列研究。
共纳入 75 例患者,中位(四分位间距(IQR))年龄为 62(53-72)岁,肥胖(47%)、高血压(67%)和糖尿病(37%)的发生率较高。与医疗保健相关的感染占 35%。第 1 天序贯器官衰竭评估(SOFA)评分的中位数(IQR)为 6(3-7)。57%的患者接受了有创机械通气(IMV),中位(IQR)时间为 11(5-22)天。接受 IMV 的患者的特征为中度降低的氧分压:吸入氧分数(第 1 天 PaO:FO = 177 [138-276];第 10 天 = 173 [147-227])和顺应性(第 1 天 = 48 [38-58] mL/cmH2O;第 10 天 = 34 [28-42] mL/cmH2O),死腔分数非常高(第 1 天 = 0.60 [0.53-0.67];第 10 天 = 0.72 [0.69-0.79])。总体住院死亡率为 25%,IMV 患者为 21%。80 岁以上患者的死亡率为 82%。
蒙特利尔 COVID-19 重症患者的特征和结局与现有文献报道的相似。我们发现生理死腔增加,这支持了肺血管损伤可能是 COVID-19 引起肺损伤的核心假说。