Division of General Internal Medicine, Department of Medicine, University of Pittsburgh School of Medicine.
Department of Pharmacy and Therapeutics, University of Pittsburgh School of Pharmacy, Pittsburgh.
Curr Opin Nephrol Hypertens. 2020 Nov;29(6):671-680. doi: 10.1097/MNH.0000000000000646.
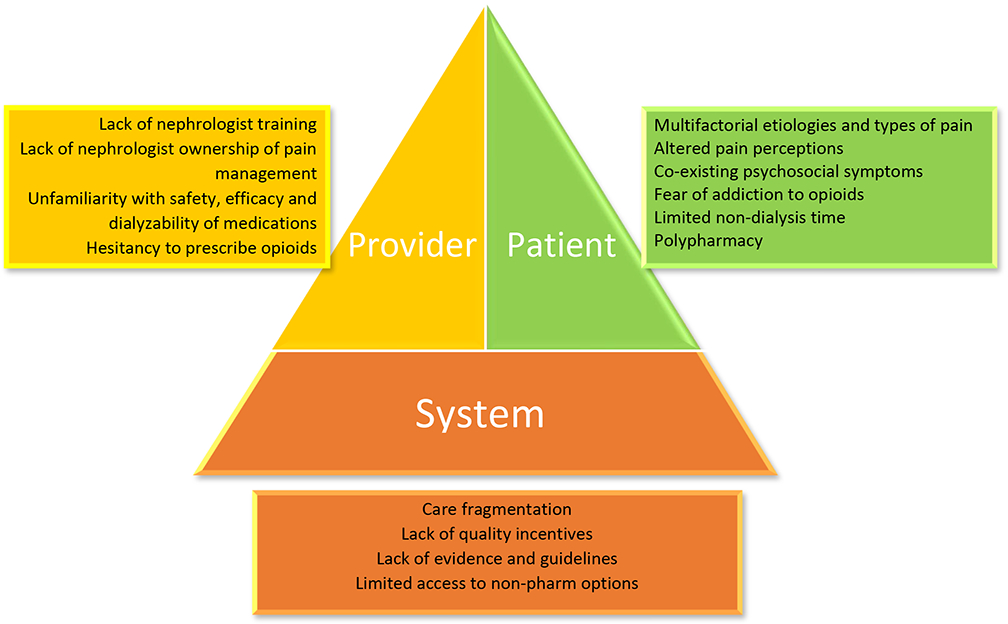
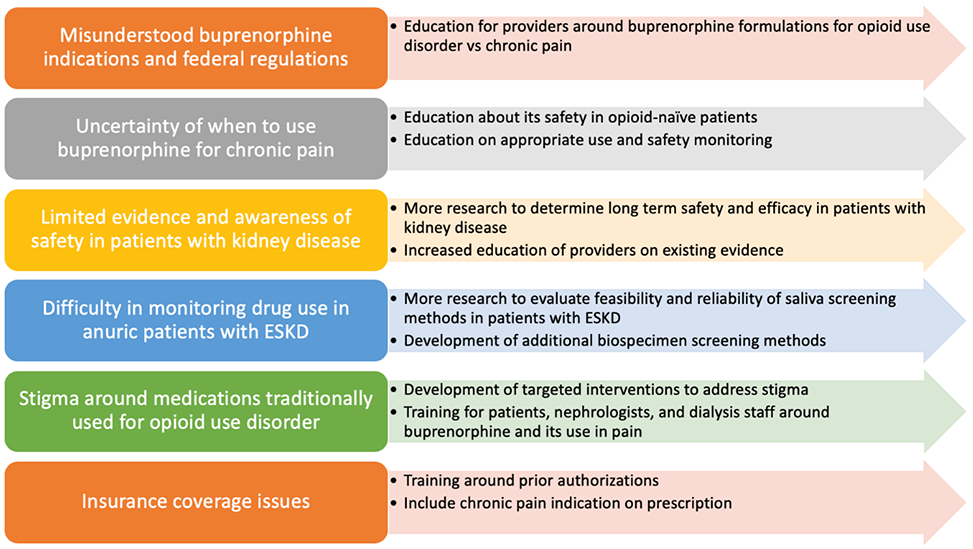
This review evaluates current recommendations for pain management in chronic kidney disease (CKD) and end-stage kidney disease (ESKD) with a specific focus on evidence for opioid analgesia, including the partial agonist, buprenorphine.
Recent evidence supports the use of physical activity and other nonpharmacologic therapies, either alone or with pharmacological therapies, for pain management. Nonopioid analgesics, including acetaminophen, topical analgesics, gabapentinoids, serotonin-norepinephrine reuptake inhibitors, and TCA may be considered based on pain cause and type, with careful dose considerations in kidney disease. NSAIDs may be used in CKD and ESKD for short durations with careful monitoring. Opioid use should be minimized and reserved for patients who have failed other therapies. Opioids have been associated with increased adverse events in this population, and thus should be used cautiously after risk/benefit discussion with the patient. Opioids that are safer to use in kidney disease include oxycodone, hydromorphone, fentanyl, methadone, and buprenorphine. Buprenorphine appears to be a promising and safer option due to its partial agonism at the mu opioid receptor.
Pain is poorly managed in patients with kidney disease. Nonpharmacological and nonopioid analgesics should be first-line approaches for pain management. Opioid use should be minimized with careful monitoring and dose adjustment.
本篇综述评估了慢性肾脏病(CKD)和终末期肾病(ESKD)患者疼痛管理的现行建议,特别关注包括部分激动剂丁丙诺啡在内的阿片类镇痛药的证据。
近期证据支持单独或联合药物治疗使用身体活动和其他非药物疗法来进行疼痛管理。非阿片类镇痛药,包括对乙酰氨基酚、局部镇痛药、加巴喷丁类、去甲肾上腺素-血清素再摄取抑制剂和三环类抗抑郁药,可根据疼痛原因和类型考虑使用,在肾脏病中要谨慎考虑剂量。在 CKD 和 ESKD 中,短期使用 NSAIDs 时应密切监测。应尽量减少阿片类药物的使用,并将其保留给其他治疗方法失败的患者。在该人群中,阿片类药物与不良反应增加相关,因此在与患者进行风险/获益讨论后,应谨慎使用。在肾脏病中更安全使用的阿片类药物包括羟考酮、氢吗啡酮、芬太尼、美沙酮和丁丙诺啡。由于丁丙诺啡对μ阿片受体具有部分激动作用,因此它似乎是一种有前途且更安全的选择。
肾脏病患者的疼痛管理不佳。非药物和非阿片类镇痛药应作为疼痛管理的一线方法。应谨慎监测和调整剂量,尽量减少阿片类药物的使用。