Xiyuan Hospital, China Academy of Chinese Medical Sciences, No.1 Xiyuan Caochang, Haidian District, Beijing, 100091, China.
Graduate School, China Academy of Chinese Medical Sciences, No. 16 Nanxiao Street, Dongzhimen, Dongcheng District, Beijing, 100700, China.
Sci Rep. 2020 Sep 18;10(1):15337. doi: 10.1038/s41598-020-72275-1.
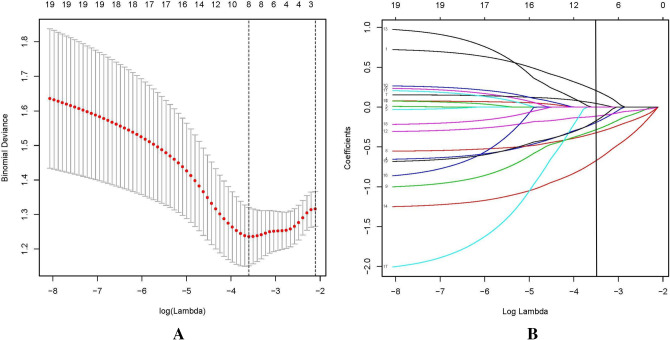
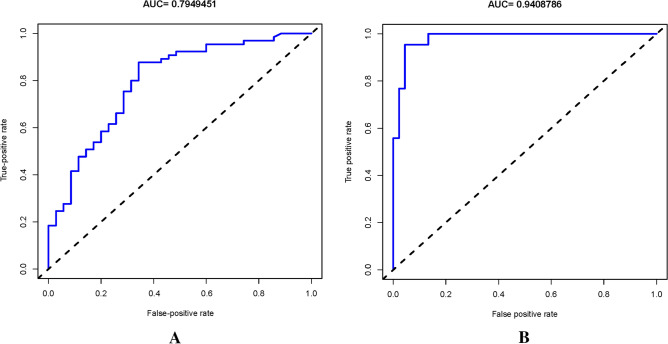
The aim of this study was to develop a model that could be used to forecast the bleeding risk of ITP based on proinflammatory and anti-inflammatory factors. One hundred ITP patients were recruited to build a new predictive nomogram, another eighty-eight ITP patients were enrolled as validation cohort, and data were collected from January 2016 to January 2019. Four demographic characteristics and fifteen clinical characteristics were taken into account. Eleven cytokines (IFN-γ, IL-1, IL-4, IL-6, IL-8, IL-10, IL-17A, IL-22, IL-23, TNF-α and TGF-β) were used to study and the levels of them were detected by using a cytometric bead array (CBA) human inflammation kit. The least absolute shrinkage and selection operator regression model was used to optimize feature selection. Multivariate logistic regression analysis was applied to build a new predictive nomogram based on the results of the least absolute shrinkage and selection operator regress ion model. The application of C-index, ROC curve, calibration plot, and decision curve analyses were used to assess the discrimination, calibration, and clinical practicability of the predictive model. Bootstrapping validation was used for testing and verifying the predictive model. After feature selection, cytokines IL-1, IL-6, IL-8, IL-23 and TGF-β were excluded, cytokines IFN-γ, IL-4, IL-10, IL-17A, IL-22, TGF-β, the count of PLT and the length of time of ITP were used as predictive factors in the predictive nomogram. The model showed good discrimination with a C-index of 0.82 (95% confidence interval 0.73376-0.90 624) in training cohortn and 0.89 (95% CI 0.868, 0.902) in validation cohort, an AUC of 0.795 in training cohort, 0.94 in validation cohort and good calibration. A high C-index value of 0.66 was reached in the interval validation assessment. Decision curve analysis showed that the bleeding risk nomogram was clinically useful when intervention was decided at the possibility threshold of 16-84%. The bleeding risk model based on IFN-γ, IL-4, IL-10, IL-17A, IL-22, TGF-β, the count of PLT and the length of time of ITP could be conveniently used to predict the bleeding risk of ITP.
本研究旨在建立一个基于促炎和抗炎因子预测 ITP 出血风险的模型。招募了 100 名 ITP 患者建立新的预测列线图,另外 88 名 ITP 患者作为验证队列,数据收集自 2016 年 1 月至 2019 年 1 月。纳入 4 项人口统计学特征和 15 项临床特征。采用流式细胞术微珠阵列(CBA)人类炎症试剂盒检测 11 种细胞因子(IFN-γ、IL-1、IL-4、IL-6、IL-8、IL-10、IL-17A、IL-22、IL-23、TNF-α和 TGF-β)的水平。采用最小绝对收缩和选择算子回归模型进行特征选择优化。基于最小绝对收缩和选择算子回归模型的结果,应用多变量逻辑回归分析建立新的预测列线图。采用 C 指数、ROC 曲线、校准图和决策曲线分析评估预测模型的区分度、校准度和临床实用性。采用自举验证法对预测模型进行检验和验证。经过特征选择,排除细胞因子 IL-1、IL-6、IL-8、IL-23 和 TGF-β,细胞因子 IFN-γ、IL-4、IL-10、IL-17A、IL-22、TGF-β、血小板计数和 ITP 持续时间作为预测列线图的预测因子。模型在训练队列中显示出良好的区分度,C 指数为 0.82(95%置信区间 0.73376-0.90624),在验证队列中为 0.89(95%CI 0.868,0.902),在训练队列中的 AUC 为 0.795,在验证队列中的 AUC 为 0.94,校准良好。间隔验证评估中达到了较高的 C 指数值 0.66。决策曲线分析表明,当干预决策可能性阈值为 16-84%时,出血风险列线图具有临床实用性。基于 IFN-γ、IL-4、IL-10、IL-17A、IL-22、TGF-β、血小板计数和 ITP 持续时间的出血风险模型可方便地用于预测 ITP 的出血风险。