Arrhythmology Department, IRCCS Policlinico San Donato, San Donato Milanese, Milano, Italy.
University Cardiology Department, IRCCS Policlinico San Donato, San Donato Milanese, Milano, Italy.
Int J Cardiol. 2021 Feb 1;324:242-248. doi: 10.1016/j.ijcard.2020.09.038. Epub 2020 Sep 19.
Hydroxychloroquine (HCQ) and azithromycin (AZT) have been proposed for COVID-19 treatment. Data available in the literature reported a potential increased risk of fatal arrhythmias under these therapies. The aim of this study was to assess the effects of these drugs on QT interval and outcome in a COVID-19 population.
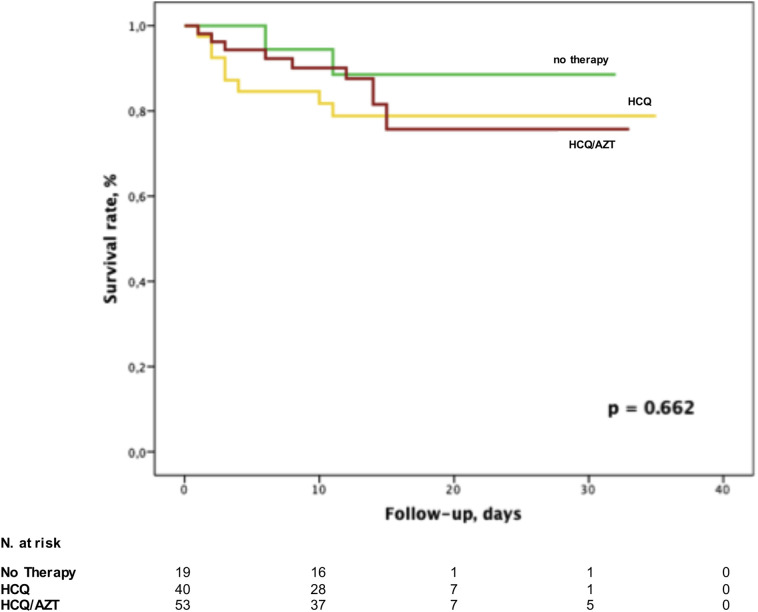
A total of 112 consecutive COVID-19 patients were included in this analysis and were divided in 3 groups according to the receiving therapeutic regimens: 19 (17%) patients in Group 1 (no treatment), 40 (36%) in Group 2 (HCQ only), 53 (47%) in Group 3 (HCQ/AZT).
A prolonged QTc interval was found in 61% of patients treated with HCQ alone or in combination with AZT, but only 4 (4%) patients showed a QTc > 500 ms. HCQ/AZT combination determined a greater increase of QTc duration compared to the other two strategies (Group 3 452 ± 26.4 vs Group 2 436.3 ± 28.4 vs Group 1 424.4 ± 24.3 ms, respectively; p < 0.001). Multivariate analysis demonstrated that HCQ/AZT combination (OR 9.02, p = 0.001) and older age (OR 1.04, p = 0.031) were independent predictors of QTc prolongation. The risk increased with age (incremental utility analysis p = 0.02). Twenty patients (18%) died, and no cardiac arrest neither arrhythmic fatalities were documented.
The HCQ/AZT combination therapy causes a significantly increase of QT interval compared to HCQ alone. Older patients under such regimen are at higher risk of experiencing QT prolongation. The use of such drugs may be considered as safe relating to arrhythmic risk in the treatment of COVID-19 patients as no arrhythmic fatalities occurred.
羟氯喹(HCQ)和阿奇霉素(AZT)已被提议用于治疗 COVID-19。文献中的现有数据报告称,这些疗法下致命性心律失常的风险可能会增加。本研究旨在评估这些药物对 COVID-19 人群 QT 间期和结局的影响。
本分析共纳入 112 例连续 COVID-19 患者,根据接受的治疗方案分为 3 组:19 例(17%)患者为 1 组(未治疗),40 例(36%)为 2 组(仅 HCQ),53 例(47%)为 3 组(HCQ/AZT)。
单独使用 HCQ 或联合 AZT 治疗的患者中,61%的患者出现 QTc 间期延长,但仅有 4 例(4%)患者出现 QTc>500ms。与其他两种策略相比,HCQ/AZT 联合使用导致 QTc 持续时间增加更大(第 3 组 452±26.4 毫秒,第 2 组 436.3±28.4 毫秒,第 1 组 424.4±24.3 毫秒;p<0.001)。多变量分析表明,HCQ/AZT 联合使用(OR 9.02,p=0.001)和年龄较大(OR 1.04,p=0.031)是 QTc 延长的独立预测因素。随着年龄的增加,风险也会增加(增量效用分析 p=0.02)。20 例(18%)患者死亡,无心脏骤停或心律失常性死亡记录。
与单独使用 HCQ 相比,HCQ/AZT 联合治疗可显著增加 QT 间期。使用该方案的老年患者发生 QT 间期延长的风险更高。在治疗 COVID-19 患者时,由于没有心律失常性死亡发生,此类药物的使用可能被认为是安全的,不会带来心律失常风险。