Student Research Committee, Health Research Center, Babol University of Medical Sciences, Babol, Iran.
Cellular and Molecular Biology Research Center, Health Research Center, Babol University of Medical Sciences, Babol, Iran.
Cardiovasc Ther. 2021 Feb 27;2021:6683098. doi: 10.1155/2021/6683098. eCollection 2021.
Hydroxychloroquine with or without azithromycin was one of the common therapies at the beginning of the COVID-19 pandemic. They can prolong QT interval, cause torsade de pointes, and lead to sudden cardiac death. We aimed to assess QT interval prolongation and its risk factors in patients who received hydroxychloroquine with or without azithromycin.
This study was a retrospective cohort study. One hundred seventy-two confirmed COVID-19 patients were included in this study, hospitalized at Babol University of Medical Sciences hospitals between , and . Patients were divided into two groups: hydroxychloroquine alone and hydroxychloroquine with azithromycin. Electrocardiograms were used for outcome assessment.
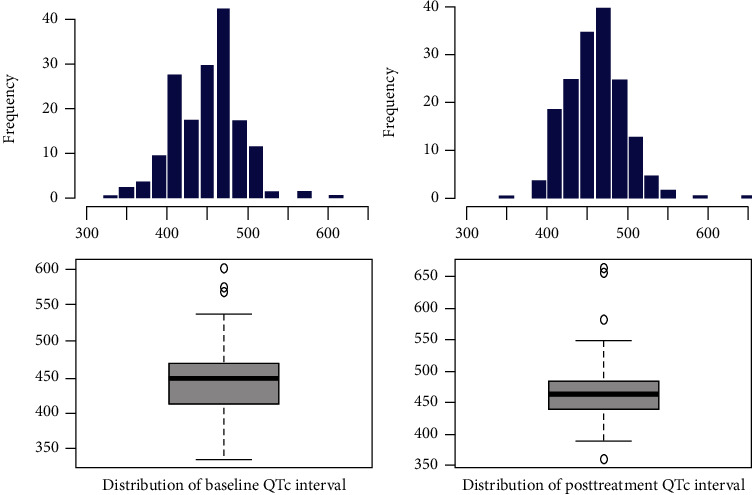
83.1% of patients received hydroxychloroquine plus azithromycin vs. 16.9% of patients who received only hydroxychloroquine. The mean age of patients was 59.2 ± 15.4.The mean of posttreatment QTc interval in the monotherapy group was shorter than the mean of posttreatment QTc interval in the combination therapy group, but it had no significant statistical difference (462.5 ± 43.1 milliseconds vs. 464.3 ± 59.1 milliseconds; = 0.488). Generally, 22.1% of patients had a prolonged QTc interval after treatment. Male gender, or baseline QTc ≥ 450 milliseconds, or high-risk Tisdale score increased the likelihood of prolonged QTc interval. Due to QTc prolongation, fourteen patients did not continue therapy after four days.
Hospitalized patients treated by hydroxychloroquine with or without azithromycin had no significant difference in prolongation of QT interval and outcome. The numbers of patients with prolonged QT intervals in this study emphasize careful cardiac monitoring during therapy, especially in high-risk patients.
羟氯喹联合或不联合阿奇霉素是 COVID-19 大流行初期的常用疗法之一。它们可延长 QT 间期,导致尖端扭转型室性心动过速,导致心源性猝死。我们旨在评估接受羟氯喹联合或不联合阿奇霉素治疗的患者的 QT 间期延长及其危险因素。
本研究为回顾性队列研究。共纳入 172 例在巴博勒医科大学附属医院确诊 COVID-19 的患者,研究时间为 2020 年 3 月至 2021 年 5 月。患者分为羟氯喹单药组和羟氯喹联合阿奇霉素组。心电图用于评估结果。
83.1%的患者接受羟氯喹联合阿奇霉素治疗,16.9%的患者仅接受羟氯喹治疗。患者的平均年龄为 59.2±15.4 岁。单药组治疗后 QTc 间期的平均值短于联合治疗组,但差异无统计学意义(462.5±43.1 毫秒 vs. 464.3±59.1 毫秒; = 0.488)。一般来说,22.1%的患者治疗后 QTc 间期延长。男性、基线 QTc≥450 毫秒或高风险 Tisdale 评分增加了 QTc 间期延长的可能性。由于 QTc 延长,14 名患者在四天后停止了治疗。
接受羟氯喹联合或不联合阿奇霉素治疗的住院患者 QT 间期延长和结局无显著差异。本研究中 QT 间期延长患者的数量强调了在治疗过程中要密切监测心脏,尤其是在高危患者中。