Hoetink Anneloes, Scherphof Sabine F, Mooi Frederik J, Westers Paul, van Dijk Jack, van de Leur Sjef J, Nierich Arno P
Department of Anesthesiology and Intensive Care, Isala, Zwolle, Netherlands.
Division of Anesthesiology Intensive Care and Emergency Medicine, University Medical Center Utrecht, Utrecht, Netherlands.
Anesthesiol Res Pract. 2020 Sep 8;2020:9584186. doi: 10.1155/2020/9584186. eCollection 2020.
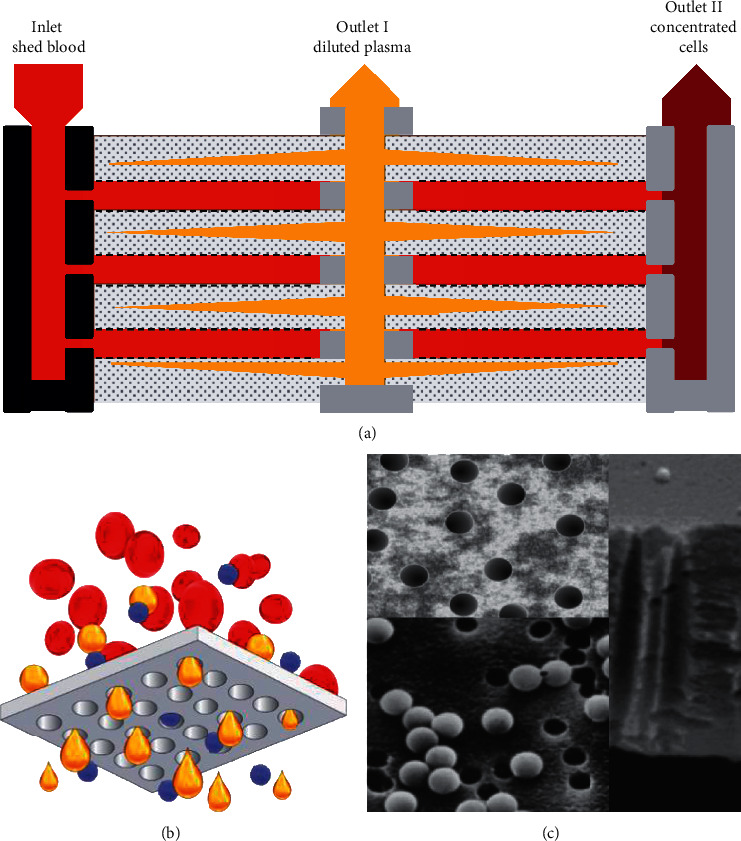
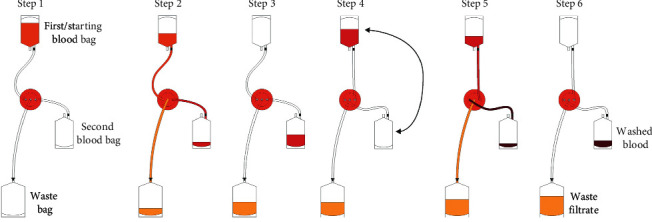
In 2013, the World Health Organization reported a shortage of 17 million red blood cell units, a number that remains growing. Acts to relieve this shortage have primarily focused on allogeneic blood collection. Nevertheless, autologous transfusion can partially alleviate the current pressure and dependence on blood banking systems. To achieve this, current gold standard autotransfusion devices should be complemented with widely available, cost-efficient, and time-efficient devices. The novel HemoClear cell salvage device (HemoClear BV, Zwolle, Netherlands), a gravity-driven microfilter, potentially is widely employable. We evaluated its performance in the cardiac postoperative setting compared to the centrifugal XTRA™ autotransfusion device.
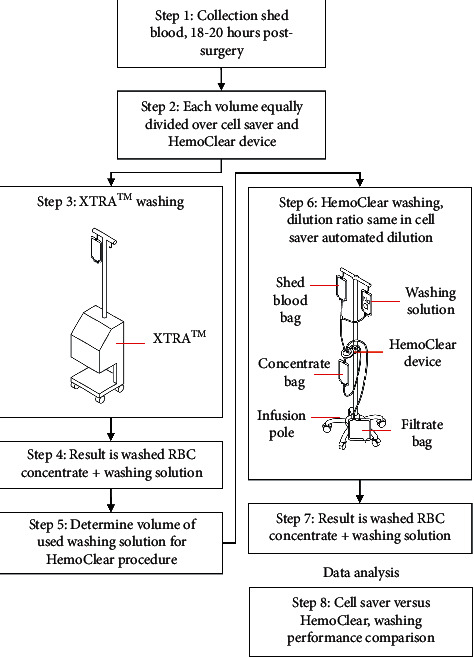
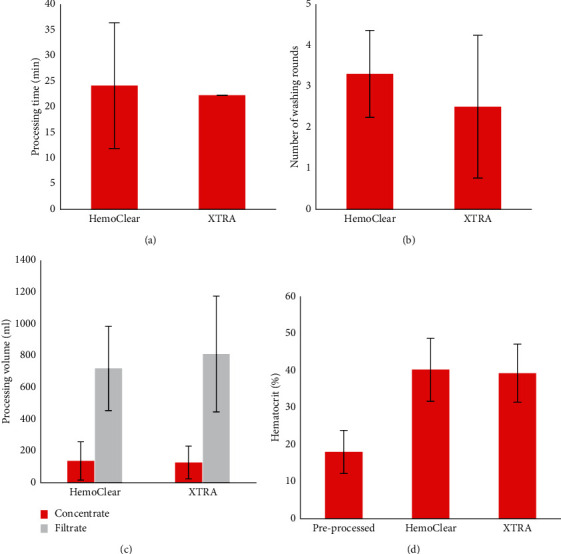
In a split-unit study ( = 18), shed blood collected 18 hours after cardiothoracic surgery was divided into two equal volumes. One-half was processed by the XTRA™ device and the other with the HemoClear blood separation system. In this paired set-up, equal washing volumes were used for both methods. Washing effectivity and cellular recovery were determined by measuring of complete blood count, free hemoglobin, complement C3, complement C4, and D-dimer in both concentrate as filtrate. Also, processing times and volumes were evaluated.
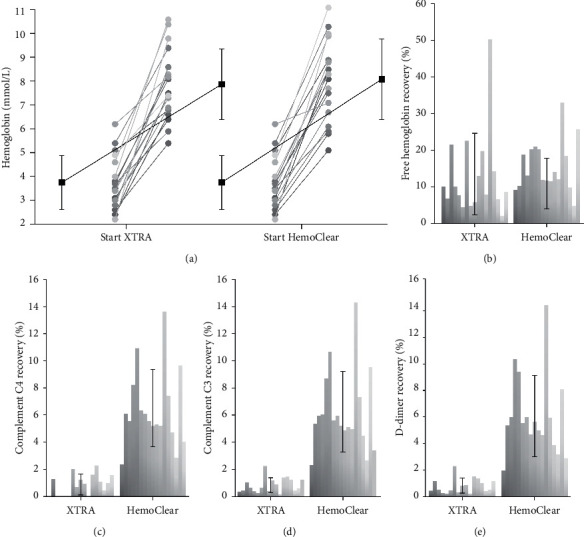
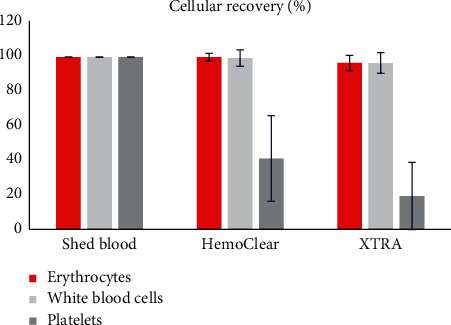
The HemoClear and XTRA™ devices showed equal effectiveness in concentrating erythrocytes and leucocytes. Both methods reduced complement C3, complement C4, and D-dimer by ≥90%. The centrifugal device reduced solutes more significantly by up to 99%. Free hemoglobin load was reduced to 12.9% and 15.5% by the XTRA™ and HemoClear, respectively.
The HemoClear device effectively produced washed concentrated red blood cells comparably to the conventional centrifugal XTRA™ autotransfusion device. Although the centrifugal XTRA™ device achieved a significantly higher reduction in contaminants, the HemoClear device achieved acceptable blood quality and seems promising in settings where gold standard cell savers are unaffordable or unpractical.
2013年,世界卫生组织报告称红细胞单位短缺1700万,且这一数字仍在增长。缓解这一短缺的行动主要集中在异体血采集上。然而,自体输血可以部分缓解当前的压力以及对血库系统的依赖。要实现这一点,当前的金标准自体输血设备应辅以广泛可用、成本效益高且省时的设备。新型HemoClear细胞回收装置(荷兰兹沃勒的HemoClear BV公司)是一种重力驱动的微滤器,具有广泛应用的潜力。我们将其在心脏术后环境中的性能与离心式XTRA™自体输血设备进行了比较。
在一项分单位研究(n = 18)中,心胸外科手术后18小时收集的引流血被分成两个相等的体积。其中一半由XTRA™设备处理,另一半由HemoClear血液分离系统处理。在这种配对设置中,两种方法使用相同的洗涤体积。通过测量浓缩物和滤液中的全血细胞计数、游离血红蛋白、补体C3、补体C4和D - 二聚体来确定洗涤效果和细胞回收率。此外,还评估了处理时间和体积。
HemoClear和XTRA™设备在浓缩红细胞和白细胞方面显示出相同的效果。两种方法都将补体C3、补体C4和D - 二聚体降低了≥90%。离心设备将溶质降低得更显著,高达99%。XTRA™和HemoClear分别将游离血红蛋白负荷降低到12.9%和15.5%。
与传统的离心式XTRA™自体输血设备相比,HemoClear设备有效地生产出了洗涤浓缩红细胞。尽管离心式XTRA™设备在减少污染物方面有显著更高的效果,但HemoClear设备达到了可接受的血液质量,并且在金标准细胞回收器无法承受或不实用的情况下似乎很有前景。