Center for Systems Biology, Massachusetts General Hospital, Harvard Medical School, Boston.
Department of Pathology, Massachusetts General Hospital, Harvard Medical School, Boston.
JAMA Netw Open. 2020 Sep 1;3(9):e2022058. doi: 10.1001/jamanetworkopen.2020.22058.
Coronavirus disease 2019 (COVID-19) is an acute respiratory illness with a high rate of hospitalization and mortality. Biomarkers are urgently needed for patient risk stratification. Red blood cell distribution width (RDW), a component of complete blood counts that reflects cellular volume variation, has been shown to be associated with elevated risk for morbidity and mortality in a wide range of diseases.
To investigate whether an association between mortality risk and elevated RDW at hospital admission and during hospitalization exists in patients with COVID-19.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study included adults diagnosed with SARS-CoV-2 infection and admitted to 1 of 4 hospitals in the Boston, Massachusetts area (Massachusetts General Hospital, Brigham and Women's Hospital, North Shore Medical Center, and Newton-Wellesley Hospital) between March 4, 2020, and April 28, 2020.
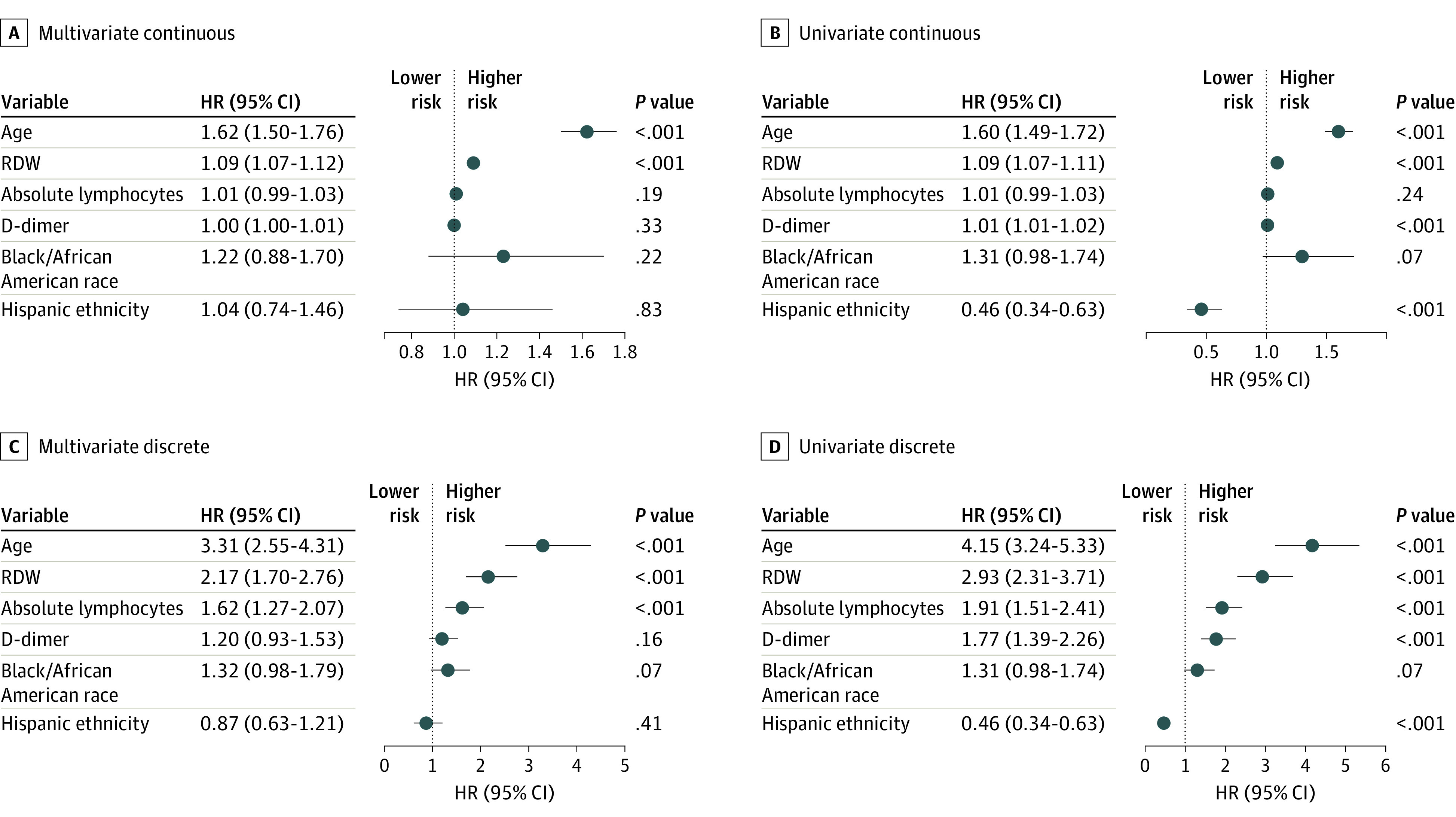
The main outcome was patient survival during hospitalization. Measures included RDW at admission and during hospitalization, with an elevated RDW defined as greater than 14.5%. Relative risk (RR) of mortality was estimated by dividing the mortality of those with an elevated RDW by the mortality of those without an elevated RDW. Mortality hazard ratios (HRs) and 95% CIs were estimated using a Cox proportional hazards model.
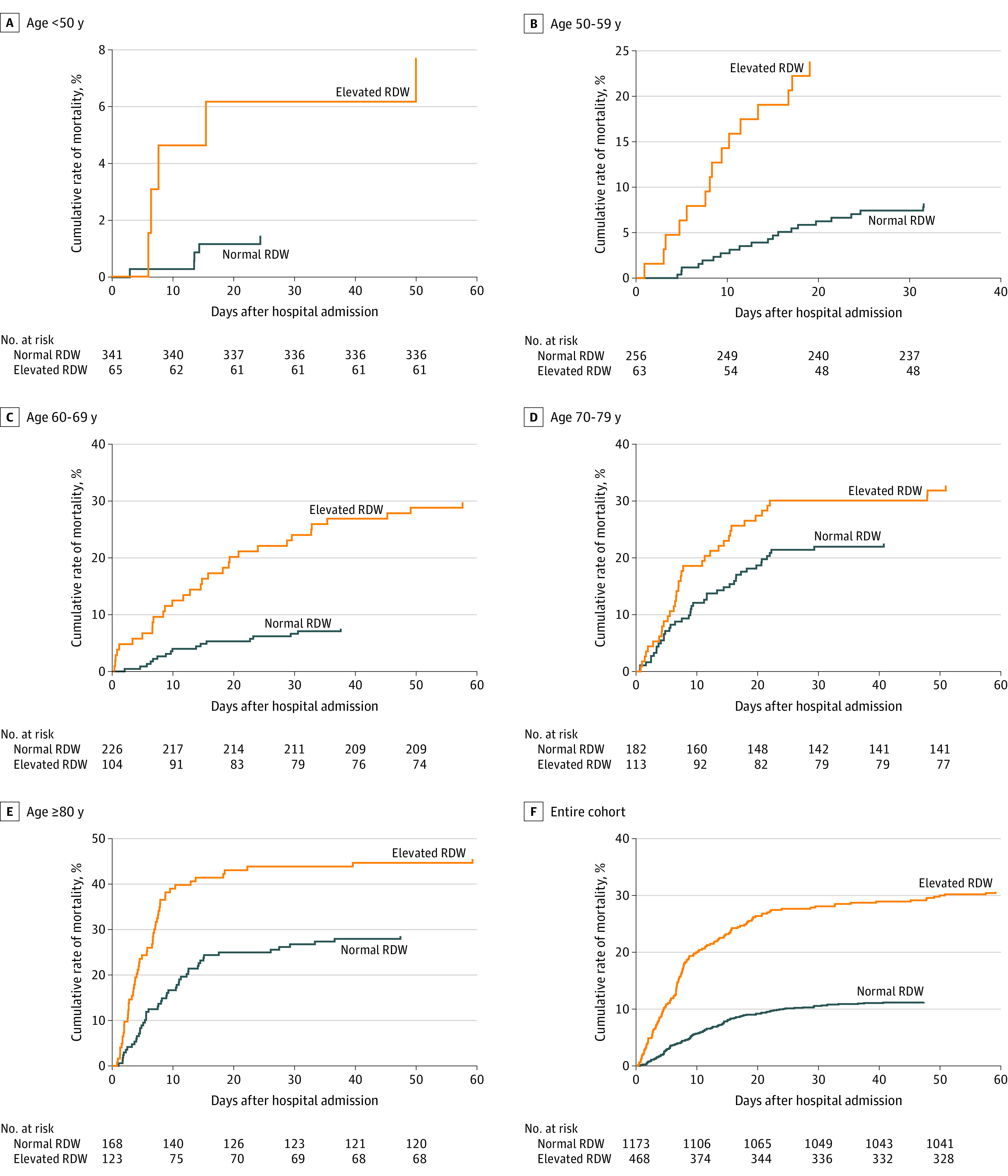
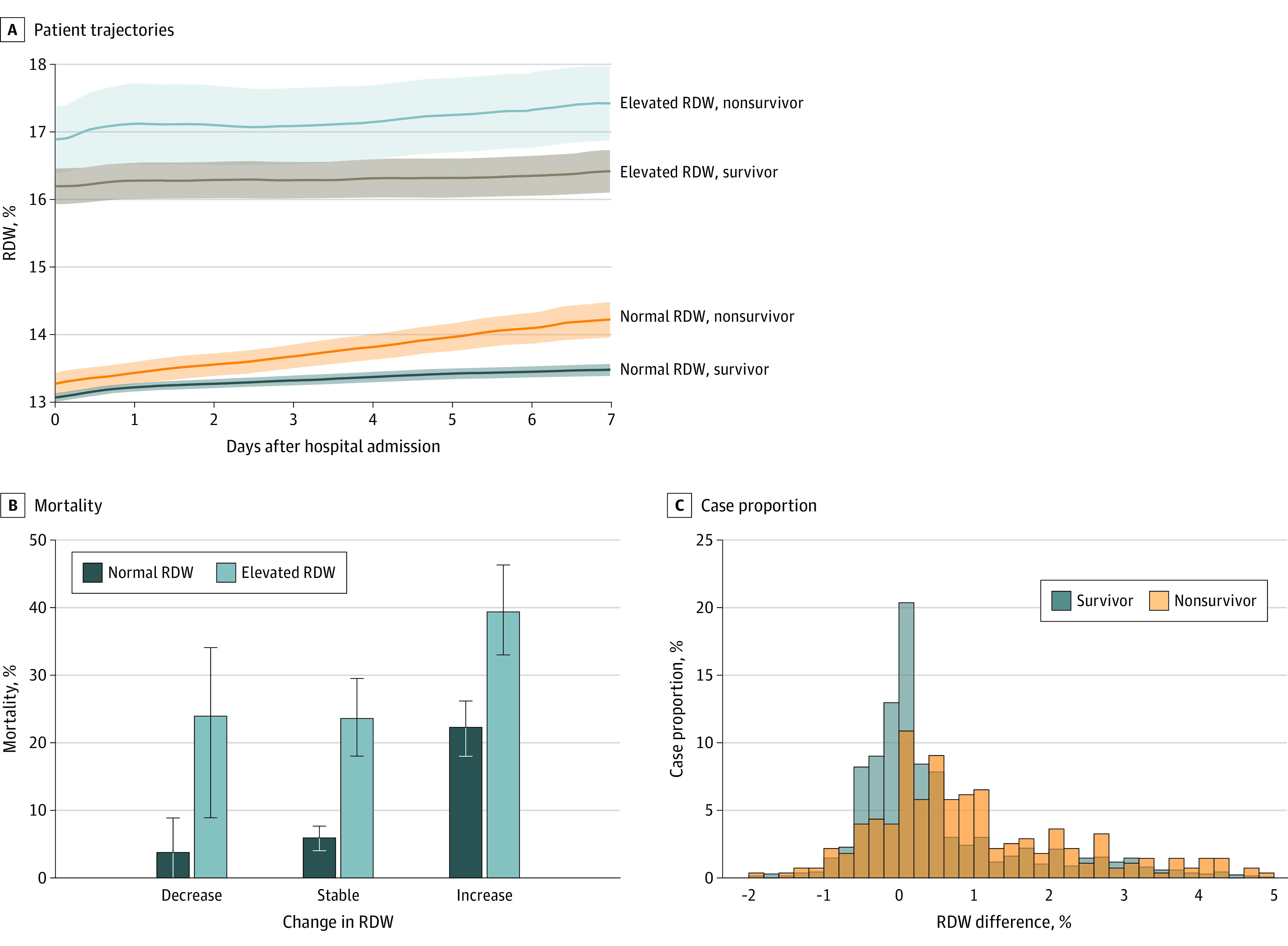
A total of 1641 patients were included in the study (mean [SD] age, 62[18] years; 886 men [54%]; 740 White individuals [45%] and 497 Hispanic individuals [30%]; 276 nonsurvivors [17%]). Elevated RDW (>14.5%) was associated with an increased mortality risk in patients of all ages. The RR for the entire cohort was 2.73, with a mortality rate of 11% in patients with normal RDW (1173) and 31% in those with an elevated RDW (468). The RR in patients younger than 50 years was 5.25 (normal RDW, 1% [n = 341]; elevated RDW, 8% [n = 65]); 2.90 in the 50- to 59-year age group (normal RDW, 8% [n = 256]; elevated RDW, 24% [n = 63]); 3.96 in the 60- to 69-year age group (normal RDW, 8% [n = 226]; elevated RDW, 30% [104]); 1.45 in the 70- to 79-year age group (normal RDW, 23% [n = 182]; elevated RDW, 33% [n = 113]); and 1.59 in those ≥80 years (normal RDW, 29% [n = 168]; elevated RDW, 46% [n = 123]). RDW was associated with mortality risk in Cox proportional hazards models adjusted for age, D-dimer (dimerized plasmin fragment D) level, absolute lymphocyte count, and common comorbidities such as diabetes and hypertension (hazard ratio of 1.09 per 0.5% RDW increase and 2.01 for an RDW >14.5% vs ≤14.5%; P < .001). Patients whose RDW increased during hospitalization had higher mortality compared with those whose RDW did not change; for those with normal RDW, mortality increased from 6% to 24%, and for those with an elevated RDW at admission, mortality increased from 22% to 40%.
Elevated RDW at the time of hospital admission and an increase in RDW during hospitalization were associated with increased mortality risk for patients with COVID-19 who received treatment at 4 hospitals in a large academic medical center network.
重要提示:COVID-19(新冠肺炎)是一种急性呼吸道疾病,其住院率和死亡率都很高。目前迫切需要生物标志物来对患者进行风险分层。红细胞分布宽度(RDW)是全血细胞计数的一个组成部分,反映了细胞体积的变化,已经证明它与广泛疾病的发病率和死亡率升高有关。
目的:研究 COVID-19 患者入院时和住院期间死亡率与升高的 RDW 之间是否存在关联。
设计、地点和参与者:这项队列研究纳入了 2020 年 3 月 4 日至 4 月 28 日期间在马萨诸塞州波士顿地区的 4 家医院(麻省总医院、布莱根妇女医院、北岸医疗中心和牛顿韦斯利医院)住院的被诊断为 SARS-CoV-2 感染的成年人。
主要结局和措施:主要结局是住院期间的患者生存率。测量指标包括入院时和住院期间的 RDW,定义升高的 RDW 大于 14.5%。通过将 RDW 升高患者的死亡率除以 RDW 正常患者的死亡率,计算死亡率的相对风险(RR)。使用 Cox 比例风险模型估计死亡率的危险比(HR)和 95%CI。
结果:共纳入 1641 例患者(平均[标准差]年龄 62[18]岁;886 名男性[54%];740 名白人[45%]和 497 名西班牙裔个体[30%];276 名非幸存者[17%])。所有年龄组患者升高的 RDW(>14.5%)与死亡率升高相关。整个队列的 RR 为 2.73,RDW 正常的患者死亡率为 11%(1173 例),RDW 升高的患者死亡率为 31%(468 例)。年龄小于 50 岁的患者 RR 为 5.25(RDW 正常,1%[n=341];RDW 升高,8%[n=65]);50 岁至 59 岁年龄组为 2.90(RDW 正常,8%[n=256];RDW 升高,24%[n=63]);60 岁至 69 岁年龄组为 3.96(RDW 正常,8%[n=226];RDW 升高,30%[n=104]);70 岁至 79 岁年龄组为 1.45(RDW 正常,23%[n=182];RDW 升高,33%[n=113]);≥80 岁年龄组为 1.59(RDW 正常,29%[n=168];RDW 升高,46%[n=123])。RDW 在调整年龄、D-二聚体(二聚体纤维蛋白原片段 D)水平、绝对淋巴细胞计数和常见合并症(如糖尿病和高血压)的 Cox 比例风险模型中与死亡率风险相关(每增加 0.5% RDW,风险比为 1.09;RDW >14.5% 与≤14.5%相比,风险比为 2.01;P<0.001)。与 RDW 未发生变化的患者相比,住院期间 RDW 增加的患者死亡率更高;RDW 正常的患者死亡率从 6%增加到 24%,而入院时 RDW 升高的患者死亡率从 22%增加到 40%。
结论和相关性:在一家大型学术医疗中心网络中接受治疗的 COVID-19 患者,入院时升高的 RDW 和住院期间 RDW 的增加与死亡率风险增加相关。