Department of Surgery, The University of Hong Kong, Hong Kong, China.
Department of Surgery, Queen Mary Hospital, Hong Kong, China.
Hepatology. 2021 Jun;73(6):2441-2454. doi: 10.1002/hep.31584. Epub 2021 May 4.
Previous recommendations suggested living donor liver transplantation (LDLT) should not be considered for patients with Model for End-Stage Liver Disease (MELD) > 25 and hepatorenal syndrome (HRS).
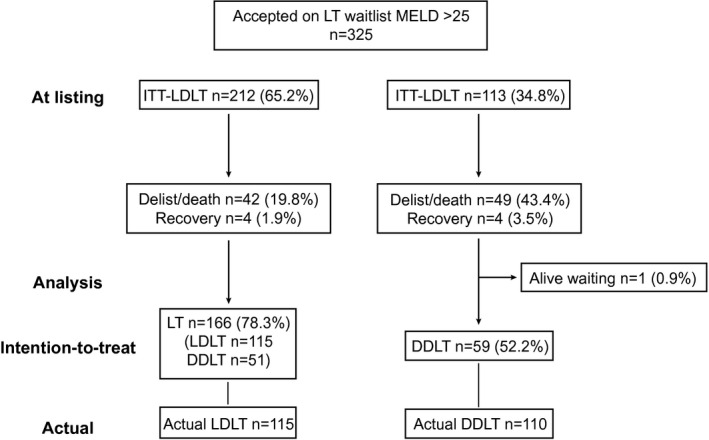
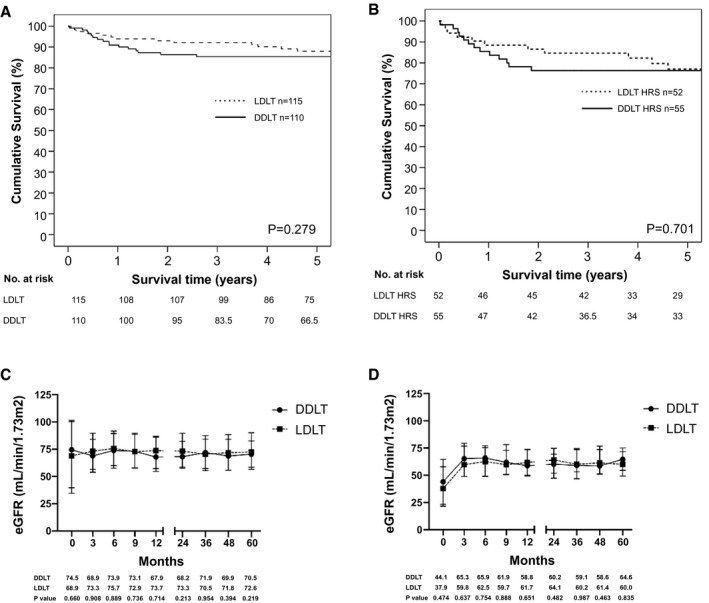
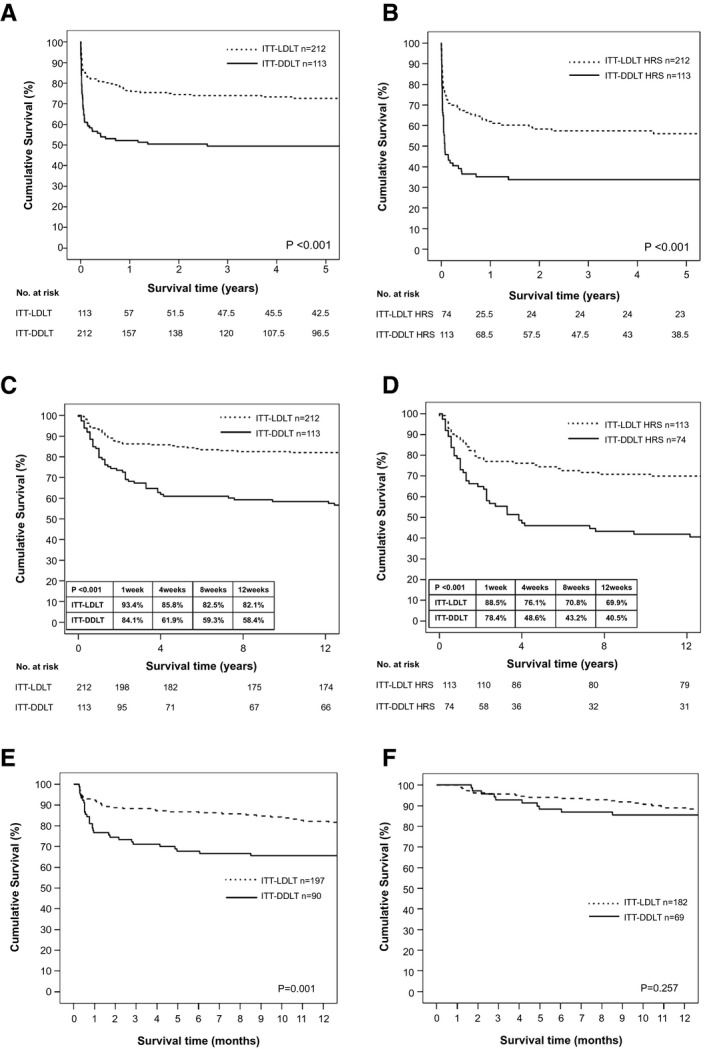
Patients who were listed with MELD > 25 from 2008 to 2017 were analyzed with intention-to-treat (ITT) basis retrospectively. Patients who had a potential live donor were analyzed as ITT-LDLT, whereas those who had none belonged to ITT-deceased donor liver transplantation (DDLT) group. ITT-overall survival (OS) was analyzed from the time of listing. Three hundred twenty-five patients were listed (ITT-LDLT n = 212, ITT-DDLT n = 113). The risk of delist/death was lower in the ITT-LDLT group (43.4% vs. 19.8%, P < 0.001), whereas the transplant rate was higher in the ITT-LDLT group (78.3% vs. 52.2%, P < 0.001). The 5-year ITT-OS was superior in the ITT-LDLT group (72.6% vs. 49.5%, P < 0.001) for patients with MELD > 25 and patients with both MELD > 25 and HRS (56% vs. 33.8%, P < 0.001). Waitlist mortality was the highest early after listing, and the distinct alteration of slope at survival curve showed that the benefits of ITT-LDLT occurred within the first month after listing. Perioperative outcomes and 5-year patient survival were comparable for patients with MELD > 25 (88% vs. 85.4%, P = 0.279) and patients with both MELD > 25 and HRS (77% vs. 76.4%, P = 0.701) after LDLT and DDLT, respectively. The LDLT group has a higher rate of renal recovery by 1 month (77.4% vs. 59.1%, P = 0.003) and 3 months (86.1% vs, 74.5%, P = 0.029), whereas the long-term estimated glomerular filtration rate (eGFR) was similar between the 2 groups. ITT-LDLT reduced the hazard of mortality (hazard ratio = 0.387-0.552) across all MELD strata.
The ITT-LDLT reduced waitlist mortality and allowed an earlier access to transplant. LDLT in patients with high MELD/HRS was feasible, and they had similar perioperative outcomes and better renal recovery, whereas the long-term survival and eGFR were comparable with DDLT. LDLT should be considered for patients with high MELD/HRS, and the application of LDLT should not be restricted with a MELD cutoff.
先前的建议认为,对于终末期肝病模型(MELD)评分>25 和肝肾综合征(HRS)的患者,不应该考虑进行活体肝移植(LDLT)。
回顾性地对 2008 年至 2017 年 MELD 评分>25 的患者进行意向治疗(ITT)分析。有潜在活体供者的患者作为 ITT-LDLT 进行分析,而没有供者的患者属于 ITT-尸体供肝移植(DDLT)组。从列入名单之日起分析 ITT 总生存(OS)。共有 325 名患者被列入名单(ITT-LDLT n=212,ITT-DDLT n=113)。ITT-LDLT 组的失访/死亡风险较低(43.4%比 19.8%,P<0.001),而 ITT-LDLT 组的移植率较高(78.3%比 52.2%,P<0.001)。对于 MELD>25 的患者和 MELD>25 且合并 HRS 的患者,ITT-LDLT 组的 5 年 ITT-OS 更优(72.6%比 49.5%,P<0.001)。等待名单死亡率在列入名单后早期最高,生存曲线斜率的明显变化表明,ITT-LDLT 的益处发生在列入名单后的第一个月内。MELD>25(88%比 85.4%,P=0.279)和 MELD>25 合并 HRS(77%比 76.4%,P=0.701)患者在 LDLT 和 DDLT 后 5 年的患者生存率相似。LDLT 组术后 1 个月(77.4%比 59.1%,P=0.003)和 3 个月(86.1%比 74.5%,P=0.029)的肾脏恢复率更高,而两组的长期估计肾小球滤过率(eGFR)相似。ITT-LDLT 降低了所有 MELD 分层的死亡率风险(风险比为 0.387-0.552)。
ITT-LDLT 降低了等待名单死亡率,并允许更早地进行移植。对于 MELD/HRS 较高的患者,LDLT 是可行的,他们具有相似的围手术期结局和更好的肾脏恢复,而长期生存和 eGFR 与 DDLT 相当。对于 MELD/HRS 较高的患者,应考虑 LDLT,并且不应该以 MELD 截断值来限制 LDLT 的应用。