IRDES, Institut de Recherche et documentation en Economie de la Santé, Paris, France.
Institut Gustave Roussy, Biostatistical and Epidemiological Division, Paris, France.
Int J Health Policy Manag. 2022 Apr 1;11(4):459-469. doi: 10.34172/ijhpm.2020.179.
The implications of competition among hospitals on care quality have been the subject of considerable debate. On one hand, economic theory suggests that when prices are regulated, quality will be increased in competitive markets. On the other hand, hospital mergers have been justified by the need to exploit cost advantages, and by evidence that hospital volume and care quality are related.
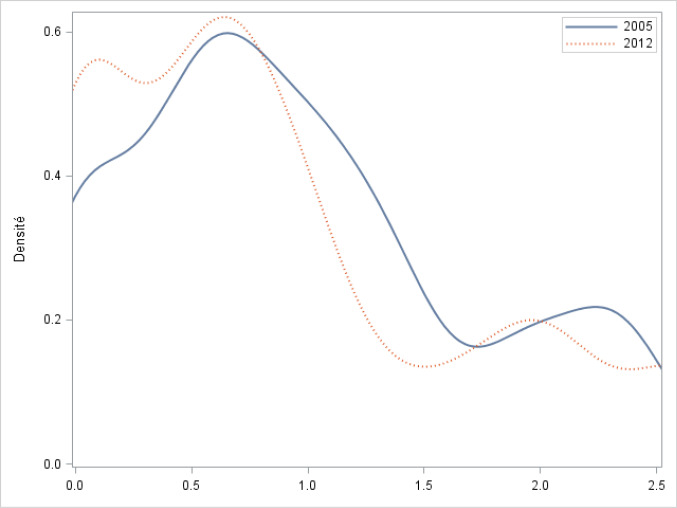
Based on patient-level data from two years (2005 and 2012) we track changes in market competition and treatment patterns in breast cancer surgery. We focus on technology adoption as a proxy of process quality and examine the likelihood of offering two innovative surgical procedures: immediate breast reconstruction (IBR), after mastectomy and sentinel lymph node biopsy (SLNB). We use an index of competition based on a multinomial logit model of hospital choice which is not subject to endogeneity bias, and estimate its impact on the propensity to receive IBR and SLNB by means of multilevel models taking into account both observable patient and hospital characteristics.
The likelihood of receiving these procedures is significantly higher in hospitals located in more competitive markets. Yet, hospital volume remains a significant indicator of quality, therefore benefits of competition appear to be sensitive to the estimates of the impact of volume on care process. In France, the centralisation policy, with minimum activity thresholds, have contributed to improving breast cancer treatment between 2005 and 2012.
Finding the right balance between costs and benefits of market competition versus concentration of hospital care supply is complex. We find that close to monopolistic markets do not encourage innovation and quality in cancer treatment, but highly competitive markets where many hospitals have very low activity volumes are also problematic because hospital quality is positively linked to patient volume.
医院之间的竞争对医疗质量的影响一直是一个备受争议的话题。一方面,经济理论表明,当价格受到监管时,竞争市场的质量将会提高。另一方面,医院合并被认为是利用成本优势的必要手段,并且有证据表明医院的数量和护理质量是相关的。
我们基于两年(2005 年和 2012 年)的患者水平数据,跟踪乳腺癌手术中市场竞争和治疗模式的变化。我们关注技术采用作为过程质量的代理指标,并研究提供两种创新手术的可能性:乳房重建术(IBR)和前哨淋巴结活检术(SLNB)。我们使用基于医院选择的多项逻辑回归模型的竞争指数,该指数不受内生性偏差的影响,并通过考虑到可观察的患者和医院特征的多层次模型来估计其对接受 IBR 和 SLNB 的倾向的影响。
在竞争更激烈的市场中,接受这些手术的可能性显著更高。然而,医院的数量仍然是质量的重要指标,因此竞争的好处似乎对医院数量对护理过程的影响的估计很敏感。在法国,中央集权政策,设定了最低活动门槛,有助于提高 2005 年至 2012 年期间的乳腺癌治疗水平。
在市场竞争与医院供应集中的成本和效益之间找到正确的平衡是复杂的。我们发现,接近垄断的市场不会鼓励癌症治疗的创新和质量,但竞争激烈的市场,许多医院的活动量非常低,也存在问题,因为医院质量与患者数量呈正相关。