Slooter M D, de Bruin D M, Eshuis W J, Veelo D P, van Dieren S, Gisbertz S S, van Berge Henegouwen M I
Amsterdam UMC, University of Amsterdam, Department of Surgery, Cancer Center Amsterdam, Amsterdam, the Netherlands.
Amsterdam UMC, University of Amsterdam, Department of Biomedical Engineering and Physics, Amsterdam, the Netherlands.
Dis Esophagus. 2021 May 22;34(5). doi: 10.1093/dote/doaa100.
Fluorescence angiography (FA) assesses anastomotic perfusion during esophagectomy with gastric conduit reconstruction, but its interpretation is subjective. This study evaluated time to fluorescent enhancement in the gastric conduit, with the aim to determine a threshold to predict postoperative anastomotic complications.
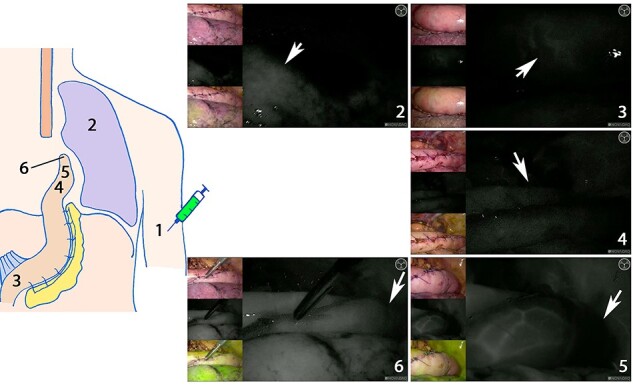
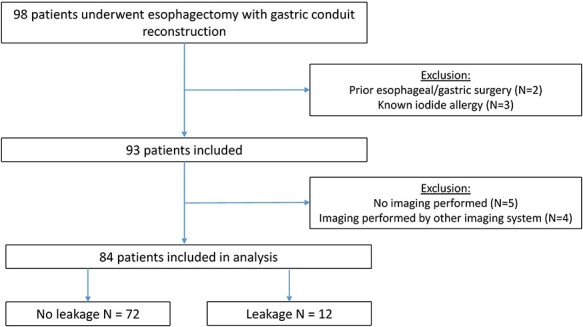
In a prospective cohort study, all consecutive patients undergoing esophagectomy with gastric conduit reconstruction from July 2018 to October 2019 were included. FA was performed before anastomotic reconstruction following injection of indocyanine green (ICG). During FA, the following time points were recorded: ICG injection, first fluorescent enhancement in the lung, at the base of the gastric conduit, at the planned anastomotic site, and at ICG watershed or in the tip of the gastric conduit. Anastomotic complications including anastomotic leakage and clinically relevant strictures were documented.
Eighty-four patients were included, the majority (67 out of 84, 80%) of which underwent an Ivor Lewis procedure. After a median follow-up of 297 days, anastomotic leakage was observed in 12 out of 84 (14.3%) and anastomotic stricture in 12 out of 82 (14.6%). Time between ICG injection and enhancement in the tip was predictive for anastomotic leakage (P = 0.174, area under the curve = 0.731), and a cut-off value of 98 seconds was derived (specificity: 98%). All times to enhancement at the planned anastomotic site and ICG watershed were significantly predictive for the occurrence of a stricture, however area under the curves were <0.7.
The identified fluorescent threshold can be used for intraoperative decision making or to identify potentially high-risk patients for anastomotic leakage after esophagectomy with gastric conduit reconstruction.
荧光血管造影(FA)用于评估胃代食管重建食管切除术中的吻合口灌注情况,但其解读具有主观性。本研究评估了胃代食管荧光增强时间,旨在确定预测术后吻合口并发症的阈值。
在一项前瞻性队列研究中,纳入了2018年7月至2019年10月期间所有连续接受胃代食管重建食管切除术的患者。在吻合口重建前注射吲哚菁绿(ICG)后进行FA。在FA过程中,记录以下时间点:ICG注射、肺部首次荧光增强、胃代食管底部、计划吻合部位、ICG分水岭处或胃代食管尖端。记录吻合口并发症,包括吻合口漏和临床相关狭窄。
共纳入84例患者,其中大多数(84例中的67例,80%)接受了艾弗·刘易斯手术。中位随访297天后,84例中有12例(14.3%)出现吻合口漏,82例中有12例(14.6%)出现吻合口狭窄。ICG注射至尖端荧光增强的时间可预测吻合口漏(P = 0.174,曲线下面积 = 0.731),得出的截断值为98秒(特异性:98%)。计划吻合部位和ICG分水岭处的所有增强时间均对狭窄的发生有显著预测作用,然而曲线下面积<0.7。
确定的荧光阈值可用于术中决策或识别胃代食管重建食管切除术后吻合口漏的潜在高危患者。