IRCCS Istituto delle Scienze Neurologiche di Bologna, Department of Neurology and Metropolitan Stroke Center, "C.A. Pizzardi" Maggiore Hospital, Largo Nigrisoli 2, 40133, Bologna, Italy.
Neurology Clinic, University of Perugia, Perugia, Italy.
Neurol Sci. 2020 Dec;41(12):3395-3399. doi: 10.1007/s10072-020-04754-2. Epub 2020 Oct 8.
A reduction of the hospitalization and reperfusion treatments was reported during COVID-19 pandemic. However, high variability in results emerged, potentially due to logistic paradigms adopted. Here, we analyze stroke code admissions, hospitalizations, and stroke belt performance for ischemic stroke patients in the metropolitan Bologna region, comparing temporal trends between 2019 and 2020 to define the impact of COVID-19 on the stroke network.
This retrospective observational study included all people admitted at the Bologna Metropolitan Stroke Center in timeframes 1 March 2019-30 April 2019 (cohort-2019) and 1 March 2020-30 April 2020 (cohort-2020). Diagnosis, treatment strategy, and timing were compared between the two cohorts to define temporal trends.
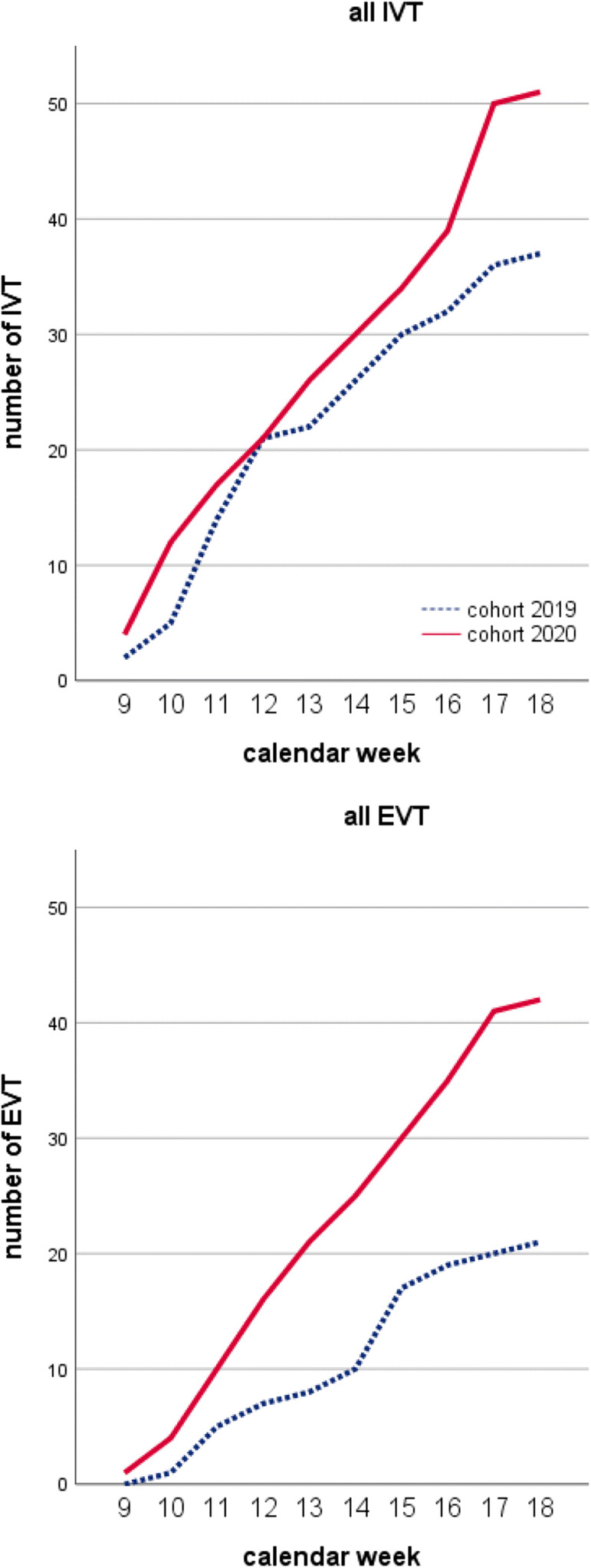
Overall, 283 patients were admitted to the Stroke Center, with no differences in demographic factors between cohort-2019 and cohort-2020. In cohort-2020, transient ischemic attack (TIA) was significantly less prevalent than 2019 (6.9% vs 14.4%, p = .04). Among 216 ischemic stroke patients, moderate-to-severe stroke was more represented in cohort-2020 (17.8% vs 6.2%, p = .027). Similar proportions of patients underwent reperfusion (45.9% in 2019 vs 53.4% in 2020), although a slight increase in combined treatment was detected (14.4% vs 25.4%, p = .05). Door-to-scan timing was significantly prolonged in 2020 compared with 2019 (28.4 ± 12.6 vs 36.7 ± 14.6, p = .03), although overall timing from stroke to treatment was preserved.
During COVID-19 pandemic, TIA and minor stroke consistently reduced compared to the same timeframe in 2019. Longer stroke-to-call and door-to-scan times, attributable to change in citizen behavior and screening at hospital arrival, did not impact on stroke-to-treatment time. Mothership model might have minimized the effects of the pandemic on the stroke care organization.
在 COVID-19 大流行期间,住院和再灌注治疗有所减少。然而,结果存在很大的差异,这可能是由于采用的逻辑范式不同。在这里,我们分析了博洛尼亚大都市区的缺血性卒中患者的卒中代码入院、住院和卒中带表现,比较了 2019 年和 2020 年的时间趋势,以确定 COVID-19 对卒中网络的影响。
这项回顾性观察性研究包括在 2019 年 3 月 1 日至 4 月 30 日(队列 2019)和 2020 年 3 月 1 日至 4 月 30 日(队列 2020)期间在博洛尼亚大都市区卒中中心入院的所有患者。比较两个队列之间的诊断、治疗策略和时间,以确定时间趋势。
总体而言,283 名患者被收入卒中中心,队列 2019 和队列 2020 之间的人口统计学因素无差异。在队列 2020 中,短暂性脑缺血发作(TIA)的发生率明显低于 2019 年(6.9% vs 14.4%,p=0.04)。在 216 例缺血性卒中患者中,中度至重度卒中在队列 2020 中更为常见(17.8% vs 6.2%,p=0.027)。接受再灌注治疗的患者比例相似(2019 年为 45.9%,2020 年为 53.4%),尽管联合治疗略有增加(14.4% vs 25.4%,p=0.05)。与 2019 年相比,2020 年的门到扫描时间明显延长(28.4±12.6 秒 vs 36.7±14.6 秒,p=0.03),尽管从卒中到治疗的总体时间保持不变。
在 COVID-19 大流行期间,与 2019 年同期相比,TIA 和轻度卒中持续减少。由于公民行为的变化和入院时的筛查,卒中到呼叫和门到扫描的时间延长,但对卒中到治疗的时间没有影响。母舰模式可能将大流行对卒中护理组织的影响降到了最低。