Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Chongqing Medical University, Chongqing, China.
Department of Critical Care Medicine, West China hospital of Sichuan University, Chengdu, Sichuan, China.
Am J Emerg Med. 2021 Aug;46:276-281. doi: 10.1016/j.ajem.2020.07.071. Epub 2020 Jul 29.
The use of high-flow nasal cannula (HFNC) and noninvasive ventilation (NIV) in patients with COVID-19 is debated.
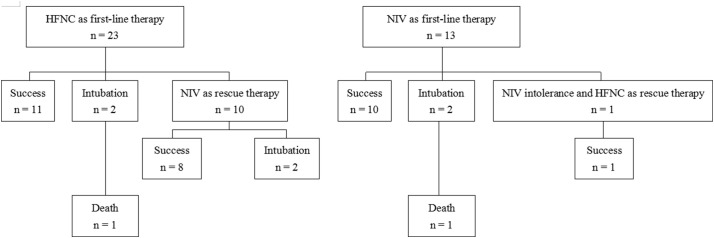
This study was performed in four hospitals of China from January to March 2020. We retrospectively enrolled 23 and 13 COVID-19 patients who used HFNC and NIV as first-line therapy, respectively.
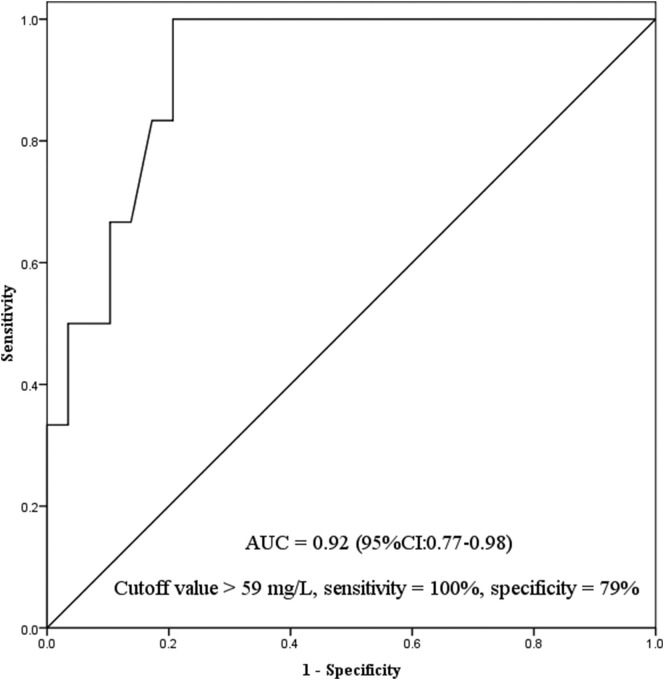
Among the 23 patients who used HFNC as first-line therapy, 10 experienced HFNC failure and used NIV as rescue therapy. Among the 13 patients who used NIV as first-line therapy, one (8%) used HFNC as rescue therapy due to NIV intolerance. The duration of HFNC + NIV (median 7.1, IQR: 3.5-12.2 vs. 7.3, IQR: 5.3-10.0 days), intubation rate (17% vs. 15%) and mortality (4% vs. 8%) did not differ between patients who used HFNC and NIV as first-line therapy. In total cohorts, 6 (17%) patients received intubation. Time from initiation of HFNC or NIV to intubation was 8.4 days (IQR: 4.4-18.5). And the time from initiation of HFNC or NIV to termination in patients without intubation was 7.1 days (IQR: 3.9-10.3). Among all the patients, C-reactive protein was independently associated with intubation (OR = 1.04, 95% CI: 1.01-1.07). In addition, no medical staff got nosocomial infection who participated in HFNC and NIV management.
In critically ill patients with COVID-19 who used HFNC and NIV as first-line therapy, the duration of HFNC + NIV, intubation rate and mortality did not differ between two groups. And no medical staff got nosocomial infection during this study.
在 COVID-19 患者中使用高流量鼻导管(HFNC)和无创通气(NIV)存在争议。
本研究于 2020 年 1 月至 3 月在中国的四家医院进行。我们回顾性纳入了分别使用 HFNC 和 NIV 作为一线治疗的 23 例和 13 例 COVID-19 患者。
在 23 例使用 HFNC 作为一线治疗的患者中,有 10 例患者 HFNC 治疗失败并使用 NIV 作为挽救性治疗。在 13 例使用 NIV 作为一线治疗的患者中,有 1 例(8%)因不耐受 NIV 而改用 HFNC 作为挽救性治疗。使用 HFNC+NIV 的时间(中位数 7.1 天,IQR:3.5-12.2 天与 7.3 天,IQR:5.3-10.0 天)、插管率(17%与 15%)和死亡率(4%与 8%)在使用 HFNC 和 NIV 作为一线治疗的患者之间没有差异。在总队列中,有 6 例(17%)患者接受了插管。从开始使用 HFNC 或 NIV 到插管的时间为 8.4 天(IQR:4.4-18.5 天)。而在未插管的患者中,从开始使用 HFNC 或 NIV 到终止的时间为 7.1 天(IQR:3.9-10.3 天)。在所有患者中,C 反应蛋白与插管独立相关(OR=1.04,95%CI:1.01-1.07)。此外,参与 HFNC 和 NIV 管理的医务人员无一例发生医院感染。
在使用 HFNC 和 NIV 作为一线治疗的 COVID-19 危重症患者中,HFNC+NIV 的持续时间、插管率和死亡率在两组之间没有差异。并且在本研究期间,没有医务人员发生医院感染。