Chen Junru, Ni Yuchao, Sun Guangxi, Liao Banghua, Zhang Xingming, Zhao Jinge, Zhu Sha, Wang Zhipeng, Shen Pengfei, Zeng Hao
Department of Urology, Institute of Urology, West China Hospital, Sichuan University, Chengdu, China.
Front Oncol. 2020 Sep 18;10:519388. doi: 10.3389/fonc.2020.519388. eCollection 2020.
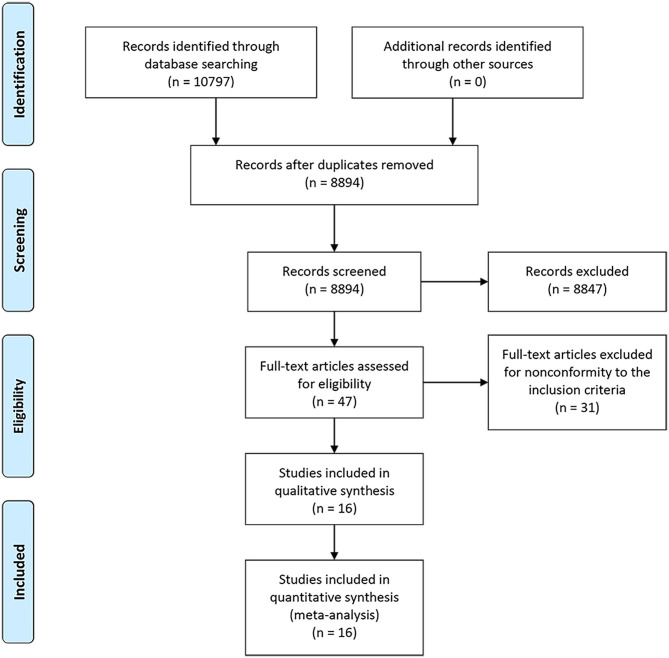
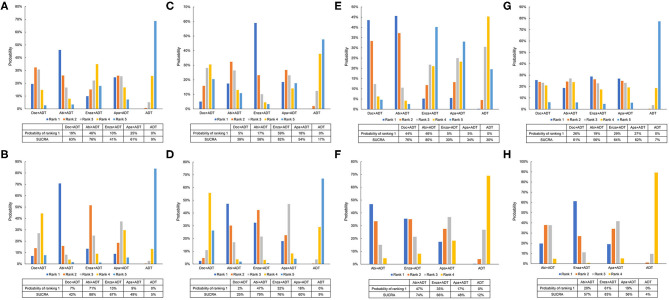
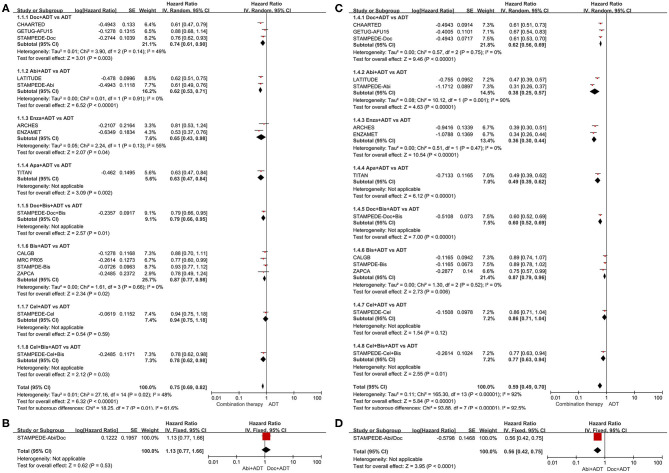
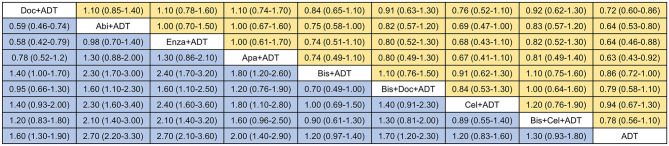
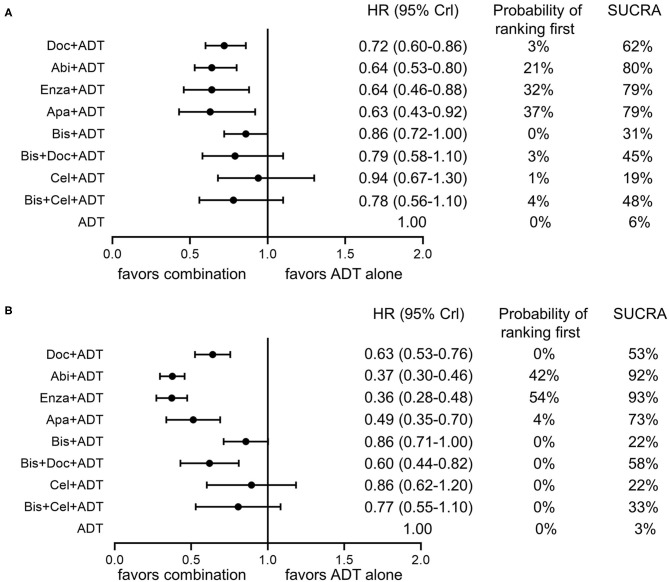
To compare the efficacy and safety of current systemic combination therapies for patients with mHSPC and help select candidates for optimal treatment. Databases of MEDLINE and EMBASE, Cochrane Central Register of Controlled Trials, and Clinical Trial.gov were searched for eligible studies. Direct and network meta-analysis were conducted to compare various systemic combination therapies and the surface under the cumulative ranking curve (SUCRA) was generated for treatment ranking. Subgroup analyses were performed according to the extent of metastasis. Adverse events (AEs) were compared among the effective treatments. Ten trials with 16 publications were included in this network meta-analysis. Direct and network meta-analysis consistently suggested that androgen-deprivation therapy (ADT) combined with docetaxel, abiraterone, enzalutamide, or apalutamide could significantly improve overall survival (OS) and failure-free survival (FFS) compared to ADT alone in men with mHSPC. SUCRA analysis demonstrated the superiority of ADT plus abiraterone or enzalutamide over other therapies. Subgroup analyses indicated that additional abiraterone to ADT had the highest ranking in patients with high-volume diseases or visceral metastases and enzalutamide plus ADT outperformed other treatments in patients with low-volume diseases or without visceral metastases. Different combination therapies had variable AE profiles and ADT in addition with docetaxel or abiraterone had the highest risk of AEs. ADT plus docetaxel, abiraterone, enzalutamide, or apalutamide were associated with significantly improved survival in patients with mHSPC. ADT plus abiraterone or enzalutamide appeared to be the most effective treatments. Clinicians should balance the efficacy, potential AEs, and disease status to select the optimal treatment.
比较当前系统性联合疗法治疗转移性去势敏感性前列腺癌(mHSPC)患者的疗效和安全性,并帮助选择最佳治疗的候选方案。检索MEDLINE、EMBASE数据库、Cochrane对照试验中央登记库和Clinical Trial.gov,以查找符合条件的研究。进行直接和网状荟萃分析,以比较各种系统性联合疗法,并生成累积排序曲线下面积(SUCRA)用于治疗排序。根据转移程度进行亚组分析。比较有效治疗组之间的不良事件(AE)。本网状荟萃分析纳入了10项试验的16篇出版物。直接和网状荟萃分析一致表明,与单纯雄激素剥夺疗法(ADT)相比,ADT联合多西他赛、阿比特龙、恩杂鲁胺或阿帕他胺可显著改善mHSPC男性患者的总生存期(OS)和无失败生存期(FFS)。SUCRA分析表明,ADT联合阿比特龙或恩杂鲁胺优于其他疗法。亚组分析表明,在高负荷疾病或内脏转移患者中,ADT联合阿比特龙的排名最高,在低负荷疾病或无内脏转移患者中,恩杂鲁胺联合ADT的疗效优于其他治疗。不同联合疗法的AE特征各不相同,ADT联合多西他赛或阿比特龙的AE风险最高。ADT联合多西他赛、阿比特龙、恩杂鲁胺或阿帕他胺可显著改善mHSPC患者的生存期。ADT联合阿比特龙或恩杂鲁胺似乎是最有效的治疗方法。临床医生应在疗效、潜在AE和疾病状态之间进行权衡,以选择最佳治疗方案。