Zizzo Gaetano, Cohen Philip L
Temple Autoimmunity Center, Lewis Katz School of Medicine at Temple University, Philadelphia, PA 19140, USA.
Unit of Rheumatology, Department of Internal Medicine, ASST Ovest Milanese, Milan, Italy.
Lancet Rheumatol. 2020 Dec;2(12):e779-e790. doi: 10.1016/S2665-9913(20)30340-4. Epub 2020 Oct 9.
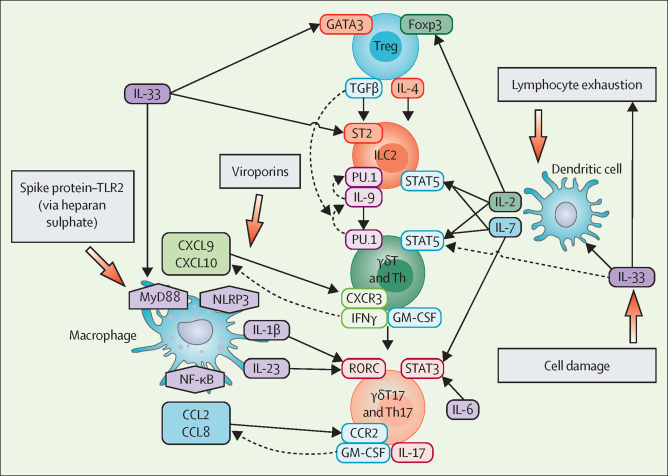
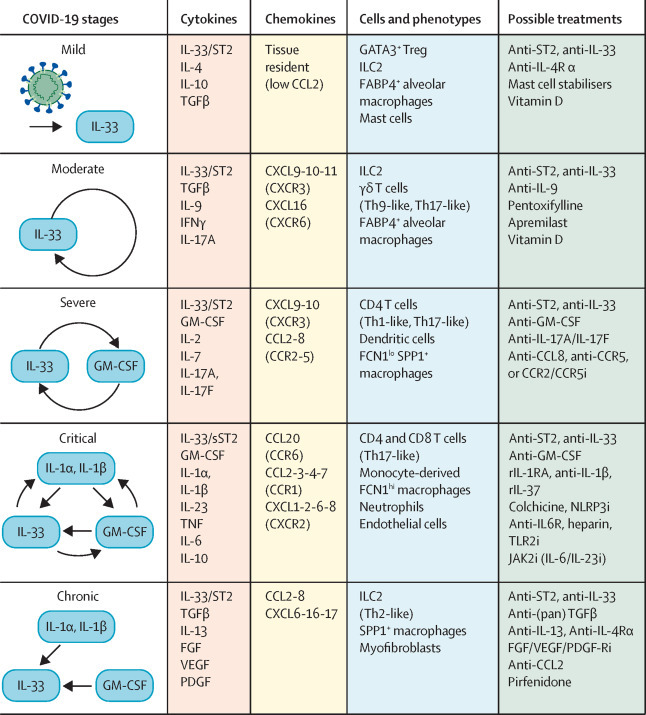
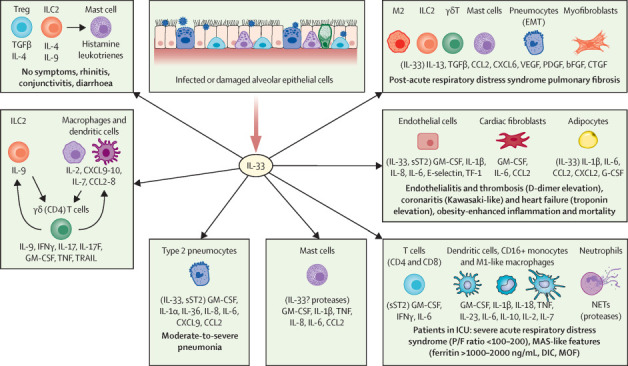
The unique cytokine signature of COVID-19 might provide clues to disease mechanisms and possible future therapies. Here, we propose a pathogenic model in which the alarmin cytokine, interleukin (IL)-33, is a key player in driving all stages of COVID-19 disease (ie, asymptomatic, mild-moderate, severe-critical, and chronic-fibrotic). In susceptible individuals, IL-33 release by damaged lower respiratory cells might induce dysregulated GATA-binding factor 3-expressing regulatory T cells, thereby breaking immune tolerance and eliciting severe acute respiratory syndrome coronavirus 2-induced autoinflammatory lung disease. Such disease might be initially sustained by IL-33-differentiated type-2 innate lymphoid cells and locally expanded γδ T cells. In severe COVID-19 cases, the IL-33-ST2 axis might act to expand the number of pathogenic granulocyte-macrophage colony-stimulating factor-expressing T cells, dampen antiviral interferon responses, elicit hyperinflammation, and favour thromboses. In patients who survive severe COVID-19, IL-33 might drive pulmonary fibrosis by inducing myofibroblasts and epithelial-mesenchymal transition. We discuss the therapeutic implications of these hypothetical pathways, including use of therapies that target IL-33 (eg, anti-ST2), T helper 17-like γδ T cells, immune cell homing, and cytokine balance.
新型冠状病毒肺炎(COVID-19)独特的细胞因子特征可能为疾病机制及未来潜在治疗方法提供线索。在此,我们提出一种致病模型,其中警报素细胞因子白细胞介素(IL)-33是驱动COVID-19疾病各个阶段(即无症状、轻中度、重度-危重症和慢性-纤维化阶段)的关键因素。在易感个体中,受损的下呼吸道细胞释放的IL-33可能诱导表达失调的GATA结合因子3的调节性T细胞,从而打破免疫耐受并引发严重急性呼吸综合征冠状病毒2诱导的自身炎症性肺病。此类疾病最初可能由IL-33分化的2型固有淋巴细胞和局部扩增的γδT细胞维持。在重症COVID-19病例中,IL-33-ST2轴可能促使表达致病粒细胞-巨噬细胞集落刺激因子的T细胞数量增加,抑制抗病毒干扰素反应,引发过度炎症,并促进血栓形成。在重症COVID-19存活患者中,IL-33可能通过诱导肌成纤维细胞和上皮-间质转化来驱动肺纤维化。我们讨论了这些假设途径的治疗意义,包括使用靶向IL-33的疗法(如抗ST2)、辅助性T细胞17样γδT细胞、免疫细胞归巢和细胞因子平衡。