Institute for Emergency Medicine, University-Hospital Schleswig-Holstein, Arnold-Heller-Str. 3, 24105, Kiel, Germany.
Division of Prehospital Services, Oslo University Hospital, Oslo, Norway.
Scand J Trauma Resusc Emerg Med. 2020 Oct 19;28(1):103. doi: 10.1186/s13049-020-00798-7.
Variation in the incidence, survival rate and factors associated with survival after cardiac arrest in Europe is reported. Some studies have tried to fill the knowledge gap regarding the epidemiology of out-of-hospital cardiac arrest in Europe but were unable to identify reasons for the reported differences. Therefore, the purpose of this study was to describe European Emergency Medical Systems, particularly from the perspective of country and ambulance service characteristics, cardiac arrest identification, dispatch, treatment, and monitoring.
An online questionnaire with 51 questions about ambulance and dispatch characteristics, on-scene management of cardiac arrest and the availability and dataset in cardiac arrest registries, was sent to all national coordinators who participated in the European Registry of Cardiac Arrest studies. In addition, individual invitations were sent to the remaining European countries.
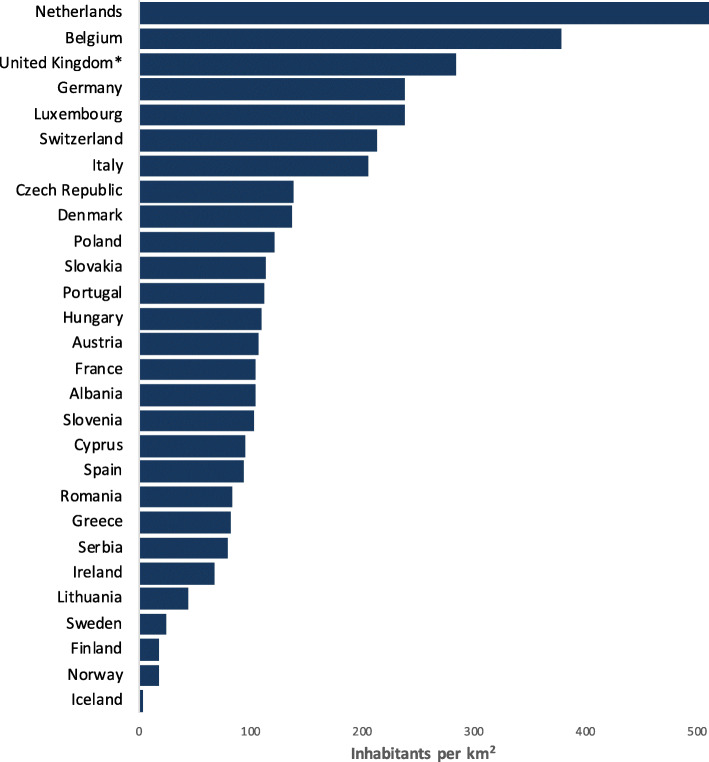
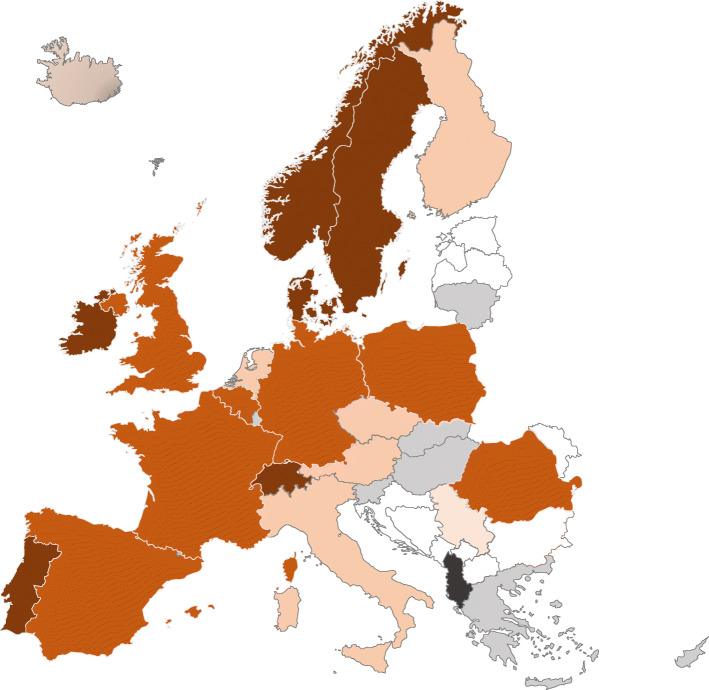
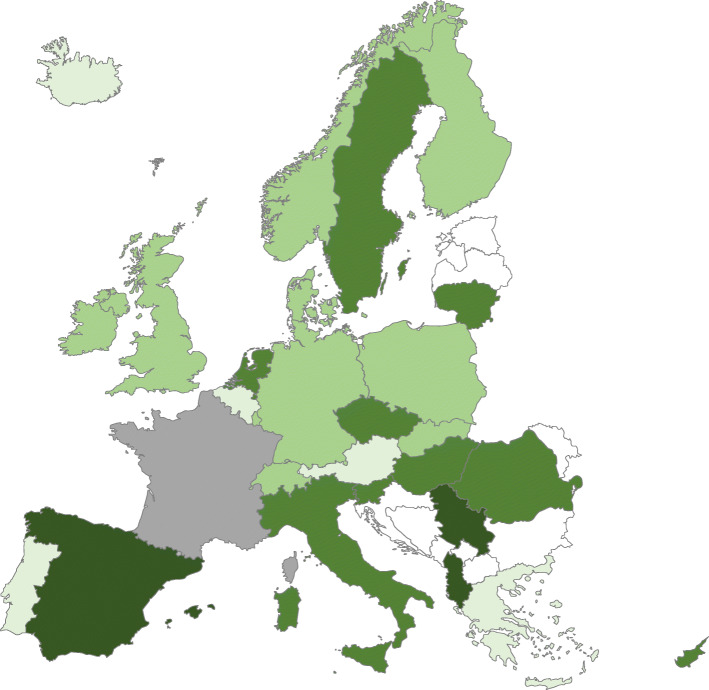
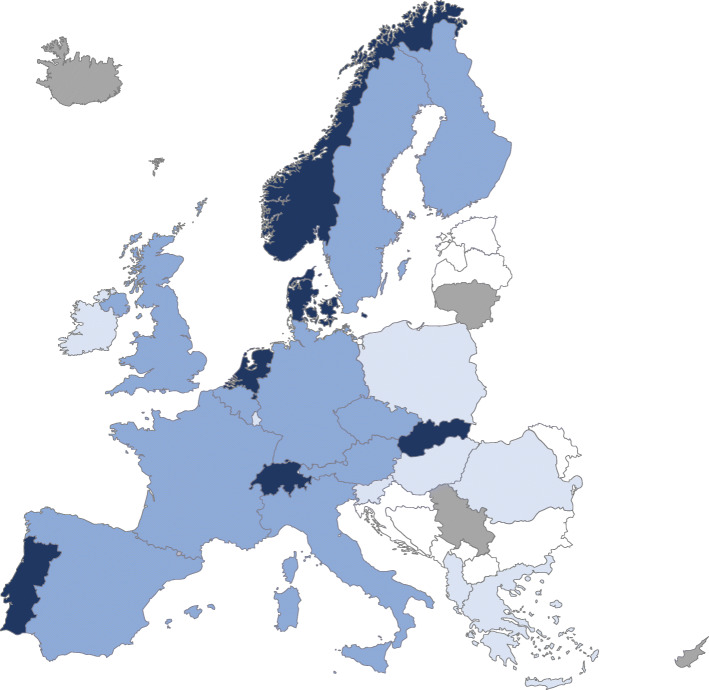
Participants from 28 European countries responded to the questionnaire. Results were combined with official information on population density. Overall, the number of Emergency Medical Service missions, level of training of personnel, availability of Helicopter Emergency Medical Services and the involvement of first responders varied across and within countries. There were similarities in team training, availability of key resuscitation equipment and permission for ongoing performance of cardiopulmonary resuscitation during transported. The quality of reporting to cardiac arrest registries varied, as well as the data availability in the registries.
Throughout Europe there are important differences in Emergency Medical Service systems and the response to out-of-hospital cardiac arrest. Explaining these differences is complicated due to significant variation in how variables are reported to and used in registries.
据报道,欧洲的心脏骤停发病率、存活率以及与存活率相关的因素存在差异。一些研究试图填补欧洲院外心脏骤停流行病学方面的知识空白,但未能确定报告差异的原因。因此,本研究的目的是描述欧洲的紧急医疗服务系统,特别是从国家和救护车服务特点、心脏骤停识别、派遣、治疗和监测的角度进行描述。
向参与欧洲心脏骤停研究的所有国家协调员发送了一份包含 51 个问题的在线问卷,内容涉及救护车和派遣特点、现场心脏骤停管理以及心脏骤停登记处的可用性和数据集。此外,还向其余欧洲国家发送了个别邀请。
来自 28 个欧洲国家的参与者回答了问卷。结果与人口密度的官方信息相结合。总体而言,紧急医疗服务任务的数量、人员的培训水平、直升机紧急医疗服务的可用性以及第一反应者的参与程度在国家之间和国家内部都有所不同。在团队培训、关键复苏设备的可用性以及在转运过程中允许持续进行心肺复苏方面存在相似之处。向心脏骤停登记处报告的质量以及登记处的数据可用性存在差异。
在整个欧洲,紧急医疗服务系统以及对院外心脏骤停的反应存在重要差异。由于向登记处报告和使用变量的方式存在显著差异,因此解释这些差异变得复杂。