Department of Medicine (Oncology), Albert Einstein College of Medicine, Montefiore Medical Center, New York, 10461, USA.
Experimental Therapeutics Program, Albert Einstein Cancer Center, Albert Einstein College of Medicine, New York, 10461, USA.
Sci Rep. 2020 Oct 19;10(1):17642. doi: 10.1038/s41598-020-74631-7.
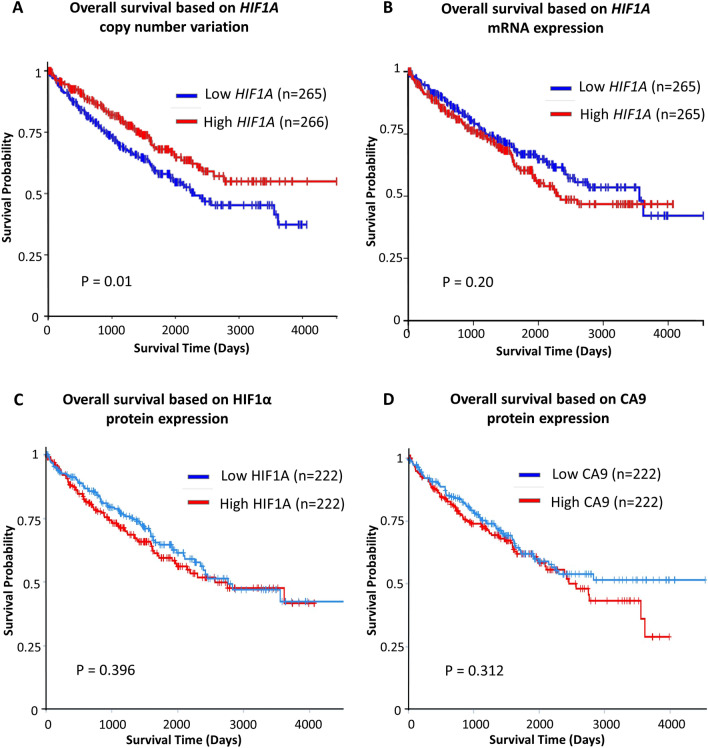
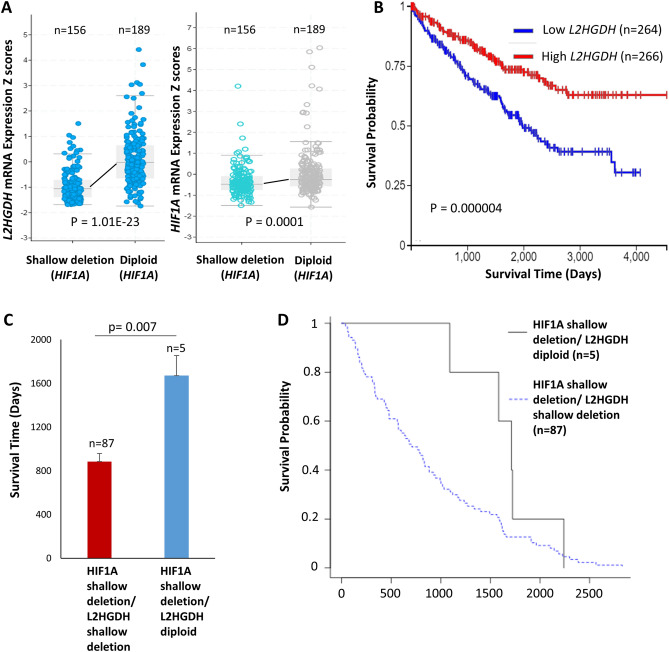
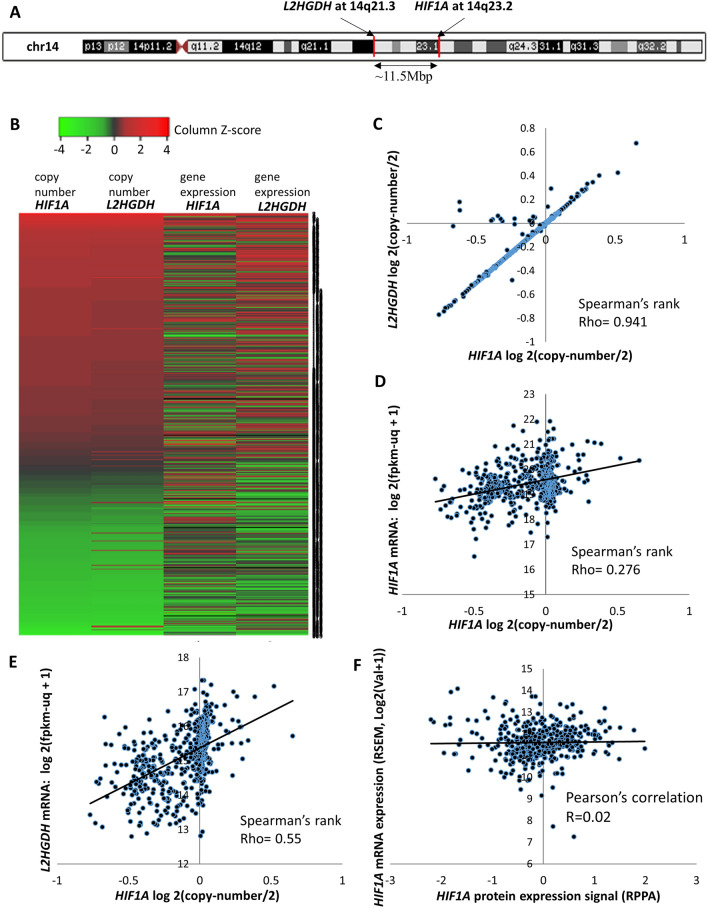
HIF1α has been termed a tumor-suppressor in clear cell renal cell carcinoma (ccRCC), primarily based on functional proliferation studies in cell lines (in vitro and in vivo) with genetic manipulation, and the adverse prognosis of 14q-deleted ccRCC patients. In other malignancies, however, HIF1α has an established tumor-promoting role. Therefore, this study sought to further examine the role of HIF1α in ccRCC using bioinformatic analyses of 530 ccRCC patients from The Cancer Genome Atlas (TCGA) and The Cancer Proteome Atlas (TCPA) registries. Although lower copy numbers of HIF1A (encoding HIF1α, located at 14q23.2) was associated with worse survival, there was no survival difference based on either HIF1A mRNA or HIF1α protein expression. Interestingly, L2HGDH (L-2-Hydroxyglutarate Dehydrogenase), a recently characterized epigenetic modulating ccRCC tumor-suppressor with a marked impact on survival, was found to be located only ~ 11.5Mbp from HIF1A on 14q (at 14q21.3). L2HGDH was therefore co-deleted in ~ 95% of 14q deletions involving HIF1A locus. Remarkably, HIF1A CNV had a markedly stronger correlation with L2HGDH expression (Rho = 0.55) than its own gene expression (Rho = 0.27), indicating high preserved-allele compensation of HIF1A. Genetic loss of HIF1A was therefore associated with a much greater reduction of L2HGDH gene expression than its own gene expression, providing a possible explanation for survival differences based on HIF1A CNV and mRNA expression. Furthermore, in 14q-deleted ccRCC patients with complete (uncensored) survival data, in the relatively rare cases where genetic loss of HIF1A occurred without genetic loss of L2HGDH (n = 5), the survival was significantly greater than where there was simultaneous genetic loss of both (n = 87) (mean survival 1670.8 ± 183.5 days vs 885.1 ± 78.4 days; p = 0.007). In addition, there was no correlation between HIF1A mRNA and HIF1α protein expression in ccRCC (R = 0.02), reflecting the primarily post-translational regulation of HIF1α. Lastly, even between L2HGDH and HIF1A loci, 14q was found to have several other yet-to-be-characterized potential ccRCC tumor-suppressors. Taken together, the data indicate that HIF1α is not a target of 14q deletion in ccRCC and that it is not a tumor-suppressor in this malignancy.
HIF1α 被称为透明细胞肾细胞癌(ccRCC)中的肿瘤抑制因子,主要基于细胞系(体外和体内)的遗传操作的功能增殖研究,以及 14q 缺失的 ccRCC 患者的不良预后。然而,在其他恶性肿瘤中,HIF1α 具有明确的促进肿瘤的作用。因此,本研究使用来自癌症基因组图谱(TCGA)和癌症蛋白质组图谱(TCPA)登记处的 530 名 ccRCC 患者的生物信息学分析,进一步研究 HIF1α 在 ccRCC 中的作用。尽管 HIF1A(编码 HIF1α,位于 14q23.2)的拷贝数较低与生存率较差相关,但无论是基于 HIF1A mRNA 还是 HIF1α 蛋白表达,生存率均无差异。有趣的是,L2HGDH(L-2-羟戊二酸脱氢酶)是最近被描述的具有明显生存影响的表观遗传调节 ccRCC 肿瘤抑制因子,其位于 14q21.3 处的 HIF1A 附近,约 11.5Mbp。因此,在涉及 HIF1A 基因座的约 95%的 14q 缺失中,L2HGDH 同时缺失。值得注意的是,HIF1A CNV 与 L2HGDH 表达(Rho = 0.55)的相关性明显强于其自身基因表达(Rho = 0.27),表明 HIF1A 的高保留等位基因补偿。因此,HIF1A 的遗传缺失与 L2HGDH 基因表达的降低幅度明显大于其自身基因表达的降低幅度,这为基于 HIF1A CNV 和 mRNA 表达的生存率差异提供了可能的解释。此外,在 14q 缺失的 ccRCC 患者中,具有完整(未删失)生存数据的患者中,在相对罕见的情况下,HIF1A 的遗传缺失发生而没有 L2HGDH 的遗传缺失(n = 5),生存率明显大于同时存在两种遗传缺失的情况(n = 87)(平均生存时间 1670.8 ± 183.5 天 vs 885.1 ± 78.4 天;p = 0.007)。此外,ccRCC 中 HIF1A mRNA 与 HIF1α 蛋白表达之间无相关性(R = 0.02),反映了 HIF1α 的主要翻译后调节。最后,即使在 L2HGDH 和 HIF1A 基因座之间,14q 也被发现具有几个尚未被表征的潜在 ccRCC 肿瘤抑制因子。综上所述,数据表明 HIF1α 不是 ccRCC 中 14q 缺失的靶标,并且在这种恶性肿瘤中不是肿瘤抑制因子。