Minniti Giuseppe, Capone Luca, Alongi Filippo, Figlia Vanessa, Nardiello Barbara, El Gawhary Randa, Scaringi Claudia, Bianciardi Federico, Tolu Barbara, Gentile Piercarlo, Paolini Sergio
Department of Medicine, Surgery and Neuroscience, Radiation Oncology Unit, University of Siena, Siena, Italy.
IRCCS Neuromed, Pozzilli (IS), Italy.
Adv Radiat Oncol. 2020 Jul 14;5(5):856-864. doi: 10.1016/j.adro.2020.06.008. eCollection 2020 Sep-Oct.
Our purpose was to assess the clinical outcomes and target positioning accuracy of frameless linear accelerator single-isocenter multiple-target (SIMT) dynamic conformal arc (DCA) stereotactic radiosurgery (SRS) for multiple brain metastases (BM).
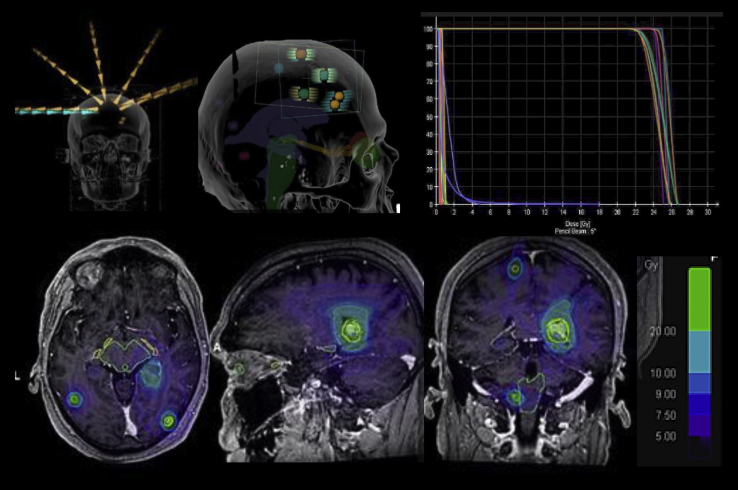
Between October 2016 and September 2018, 31 consecutive patients ≥18 years old with 204 BM <3 cm in maximum size receiving SIMT DCA SRS were retrospectively evaluated. All plans were created using a dedicated automated treatment planning software (Brainlab, Munich, Germany), and treatments were performed with a Truebeam STx or a Novalis Tx (Brainlab and Varian Medical Systems, CA). The accuracy of setup and interfraction patient repositioning was assessed by Brainlab ExacTrac radiograph 6-dimensional image system and the risk of compromised target dose coverage evaluated. Brain control and overall survival were estimated by Kaplan-Meier method calculated from the time of SRS.
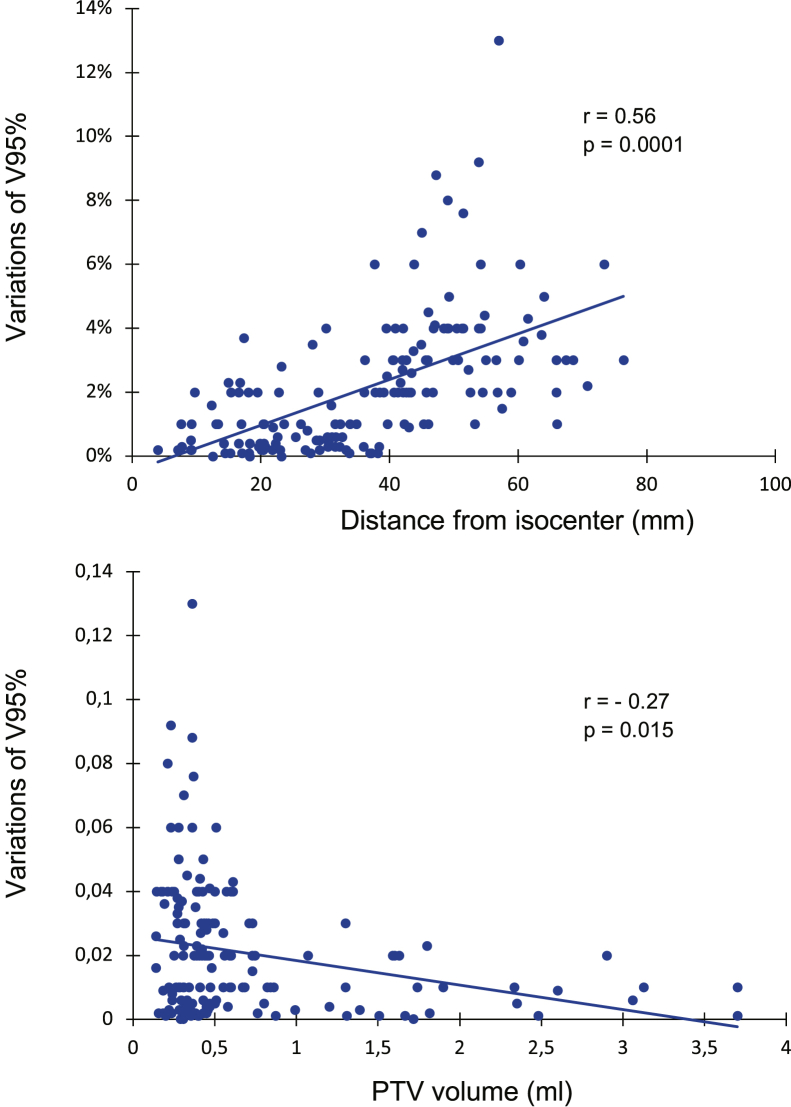
Fourteen patients were treated for 4 to 6 and 17 patients for 7 to 10 BM. The mean gross tumor volume (GTV) was 0.65 cm and the mean planning target volume (PTV) was 0.89 cm. Mean V95 (the volume of the PTV covered by 95% of the prescription dose) and D95 (the prescription dose covering 95% of the PTV) were 99.5% and 21.1 Gy, respectively. With a median clinical follow-up of 11 months (range, 4-26 months), the 1-year survival was 68% and local control was 89%. As a consequence of plan isocenter residual errors, a loss of target coverage, defined as V95 < 95%, occurred in 28 PTVs (10 patients); using a 1 mm GTV-to-PTV margin, adequate dose coverage was maintained for all lesions.
SIMT DCA SRS represents a fast and effective approach for patients with up to 10 BM. The dosimetric effects of residual set-up and intrafraction positioning errors are modest, although a GTV-to-PTV margin of 1 mm is recommended.
我们的目的是评估无框架直线加速器单等中心多靶点(SIMT)动态适形弧(DCA)立体定向放射外科(SRS)治疗多发脑转移瘤(BM)的临床疗效和靶点定位准确性。
回顾性评估2016年10月至2018年9月期间连续31例年龄≥18岁、最大直径<3 cm的204个BM接受SIMT DCA SRS治疗的患者。所有计划均使用专用的自动治疗计划软件(德国慕尼黑的Brainlab)创建,并使用Truebeam STx或Novalis Tx(Brainlab和瓦里安医疗系统公司,加利福尼亚州)进行治疗。通过Brainlab ExacTrac射线照片6维图像系统评估设置和分次间患者重新定位的准确性,并评估靶区剂量覆盖受损的风险。通过从SRS时间开始计算的Kaplan-Meier方法估计脑部控制和总生存期。
14例患者治疗4至6个BM,17例患者治疗7至10个BM。平均肿瘤总体积(GTV)为0.65 cm,平均计划靶体积(PTV)为0.89 cm。平均V95(处方剂量的95%覆盖的PTV体积)和D95(覆盖PTV的95%的处方剂量)分别为99.5%和21.1 Gy。中位临床随访11个月(范围4-26个月),1年生存率为68%,局部控制率为89%。由于计划等中心残留误差,28个PTV(10例患者)出现靶区覆盖丢失,定义为V95<95%;使用1 mm的GTV到PTV边界,所有病变均维持了足够的剂量覆盖。
SIMT DCA SRS是一种治疗多达10个BM患者的快速有效方法。尽管建议GTV到PTV边界为1 mm,但残留设置和分次内定位误差的剂量学影响较小。