Faccenda Valeria, Colciago Riccardo Ray, Bianchi Sofia Paola, De Ponti Elena, Panizza Denis, Arcangeli Stefano
Medical Physics Department, Fondazione IRCCS San Gerardo dei Tintori, 20900 Monza, Italy.
School of Medicine and Surgery, University of Milan Bicocca, 20126 Milan, Italy.
Cancers (Basel). 2024 Sep 23;16(18):3243. doi: 10.3390/cancers16183243.
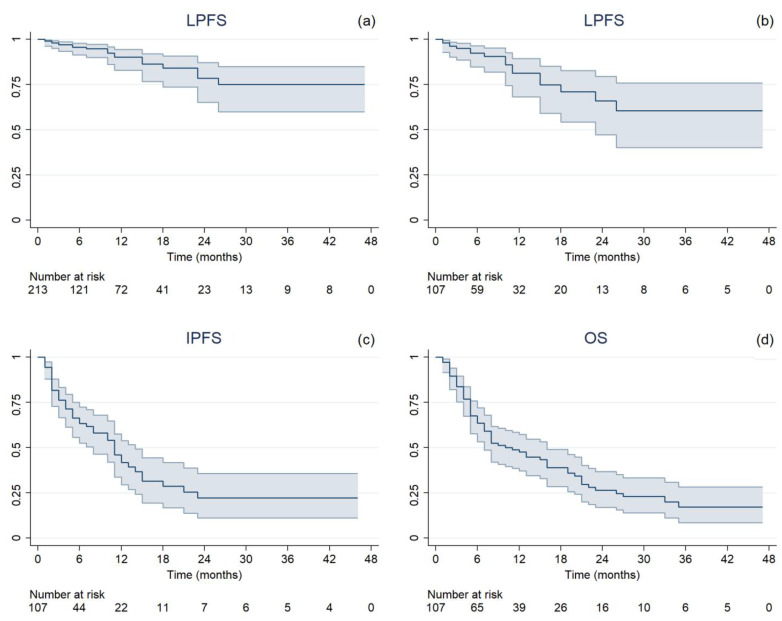
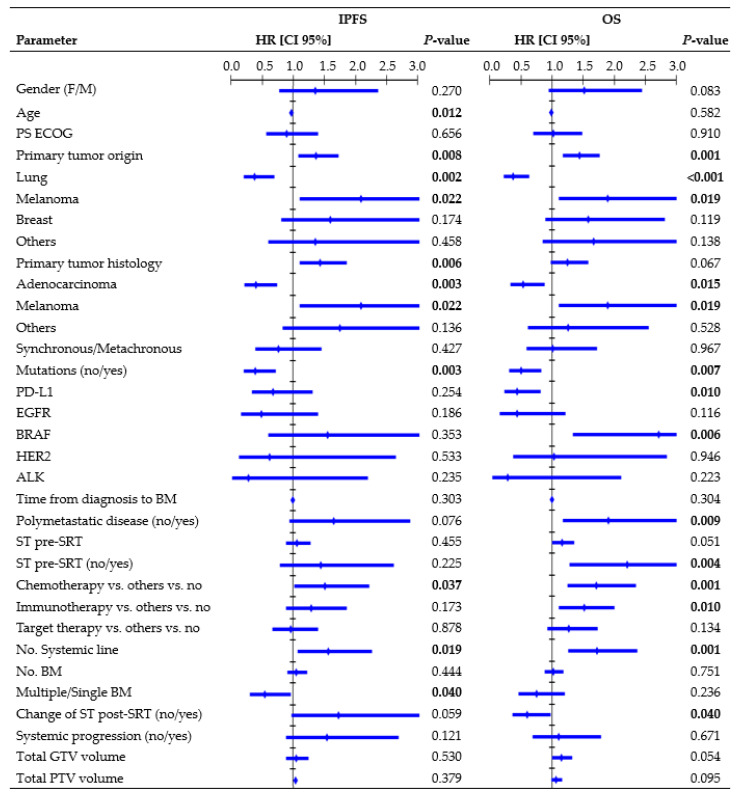
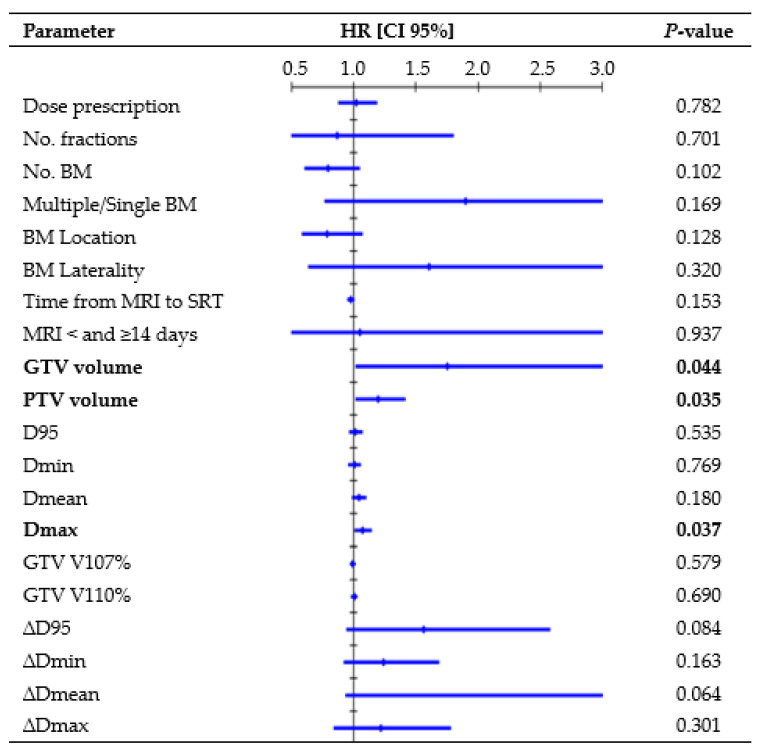
To report on predictive factors in Linac-based SRT for single and multiple BM. Consecutive patients receiving either one or three fractions of single-isocenter coplanar VMAT SRT were retrospectively included. The GTV-PTV margin was 1-2 mm. The delivered target dose was estimated by recalculating the original plans on roto-translated CT according to errors recorded by post-treatment CBCT. The Kaplan-Meier method estimated local progression-free survival (LPFS), intracranial progression-free survival (IPFS), and overall survival (OS). Log-rank and Wilcoxon-Mann-Whitney tests evaluated inter-group differences, whereas Cox regression analysis assessed prognostic factors. Fifty females and fifty males, with a median age of 69 years, received 107 SRTs. A total of 213 BM (range, 1-10 per treatment) with a median volume of 0.22 cc were irradiated with a median minimum BED of 59.5 Gy. The median delivered GTV D95 reduction was -0.3%. The median follow-up was 11 months. Nineteen LP events and a 1-year LC rate of 90.1% were observed. The GTV coverage did not correlate with LC, while the GTV volume was a risk factor for LP, with the 1-year rate dropping to 73% for volumes ≥ 0.88 cc. The median LPFS, IPFS, and OS were 6, 5, and 7 months, respectively. Multivariate analysis showed that patients with melanoma histology and those receiving a second or subsequent systemic therapy line had the worst outcomes, whereas patients with adenocarcinoma histology and mutations showed better results. The accuracy and efficacy of the Linac-based SRT approach for BM were confirmed, but the dose distribution alone failed to predict the treatment response, suggesting that other factors must be considered to maximize SRT outcomes.
报告基于直线加速器的立体定向放射治疗(SRT)对单发和多发脑转移瘤(BM)的预测因素。回顾性纳入接受单次等中心共面容积调强弧形放疗(VMAT)SRT 1次或3次分割的连续患者。大体肿瘤体积(GTV)至计划靶体积(PTV)的边界为1 - 2毫米。根据治疗后锥束CT(CBCT)记录的误差,在旋转平移CT上重新计算原始计划,从而估算出实际给予的靶区剂量。采用Kaplan - Meier法估计局部无进展生存期(LPFS)、颅内无进展生存期(IPFS)和总生存期(OS)。采用对数秩检验和Wilcoxon - Mann - Whitney检验评估组间差异,而Cox回归分析评估预后因素。50名女性和50名男性,中位年龄69岁,接受了107次SRT治疗。共照射213个BM(范围为每次治疗1 - 10个),中位体积为0.22立方厘米,中位最小生物等效剂量(BED)为59.5 Gy。实际给予的GTV D95的中位降低值为 - 0.3%。中位随访时间为11个月。观察到19例局部进展(LP)事件,1年局部控制(LC)率为90.1%。GTV覆盖情况与LC无关,而GTV体积是LP的一个危险因素,当体积≥0.88立方厘米时,1年发生率降至73%。LPFS、IPFS和OS的中位时间分别为6个月、5个月和7个月。多变量分析显示,黑色素瘤组织学类型的患者以及接受二线或后续全身治疗方案的患者预后最差,而腺癌组织学类型且有突变的患者结果较好。基于直线加速器的SRT治疗BM的准确性和有效性得到了证实,但仅剂量分布无法预测治疗反应,这表明必须考虑其他因素以优化SRT治疗效果。