Kurji Jaameeta, Gebretsadik Lakew Abebe, Wordofa Muluemebet Abera, Morankar Sudhakar, Bedru Kunuz Haji, Bulcha Gebeyehu, Bergen Nicole, Kiros Getachew, Asefa Yisalemush, Asfaw Shifera, Mamo Abebe, Endale Erko, Thavorn Kednapa, Labonte Ronald, Taljaard Monica, Kulkarni Manisha A
School of Epidemiology and Public Health, University of Ottawa, 600 Peter Morand Crescent, Ottawa, Ontario, K1G 5Z3, Canada.
Department of Health, Behaviour & Society, Jimma University, Jimma Town, Jimma Zone, Ethiopia.
BMC Public Health. 2020 Oct 22;20(1):1593. doi: 10.1186/s12889-020-09692-4.
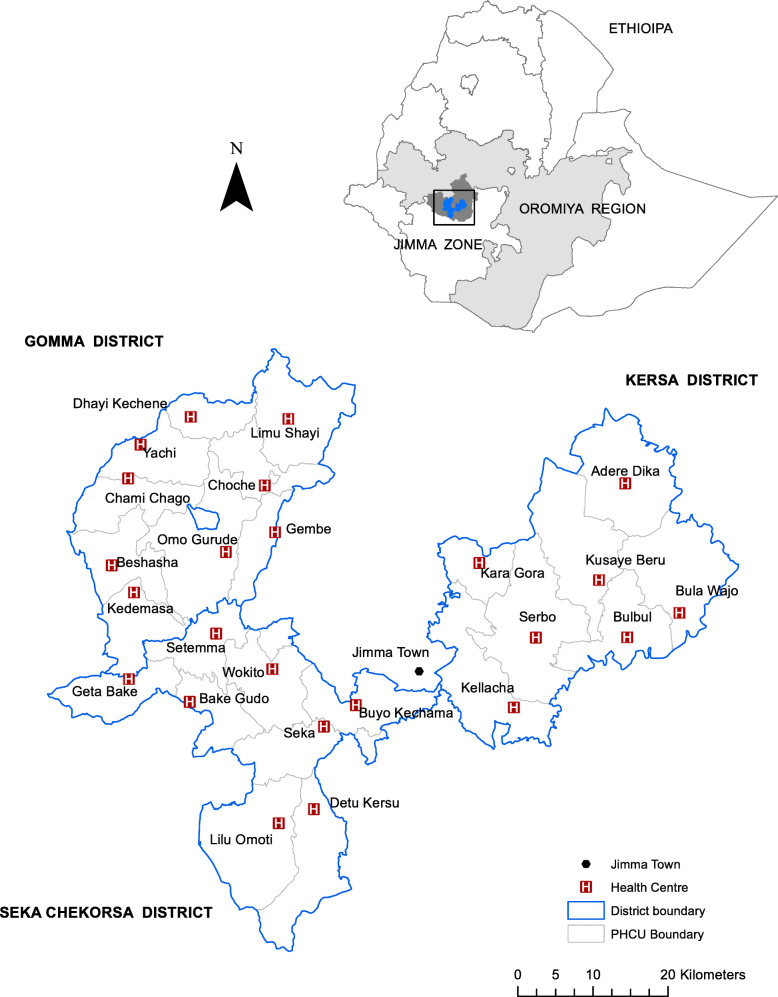
Maternity waiting homes (MWHs), residential spaces for pregnant women close to obstetric care facilities, are being used to tackle physical barriers to access. However, their effectiveness has not been rigorously assessed. The objective of this cluster randomized trial was to evaluate the effectiveness of functional MWHs combined with community mobilization by trained local leaders in improving institutional births in Jimma Zone, Ethiopia.
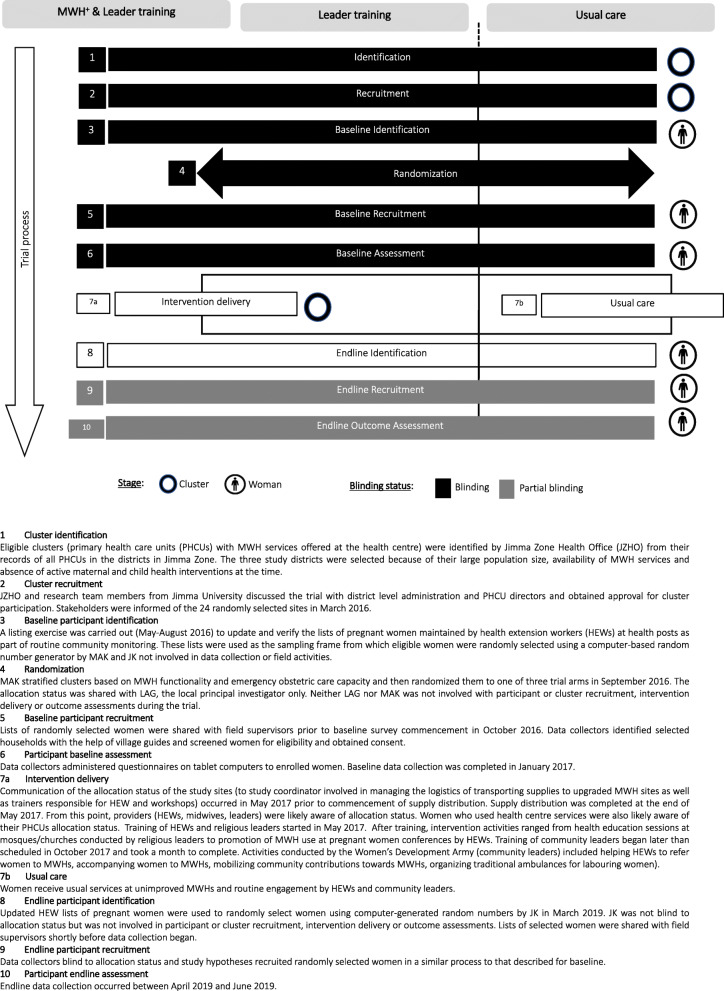
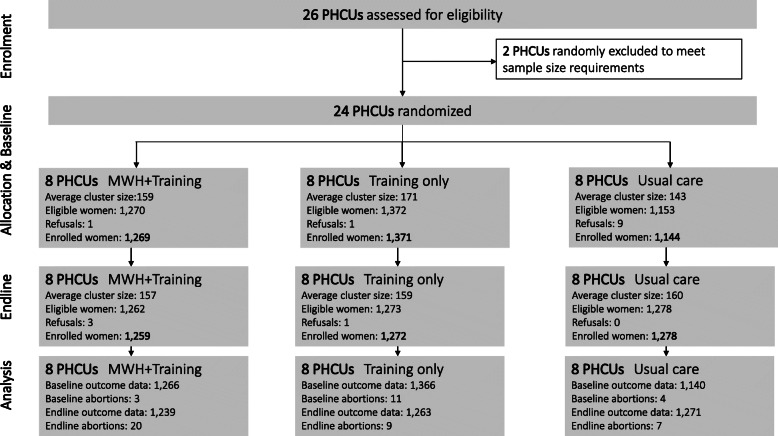
A pragmatic, parallel arm cluster-randomized trial was conducted in three districts. Twenty-four primary health care units (PHCUs) were randomly assigned to either (i) upgraded MWHs combined with local leader training on safe motherhood strategies, (ii) local leader training only, or (iii) usual care. Data were collected using repeat cross-sectional surveys at baseline and 21 months after intervention to assess the effect of intervention on the primary outcome, defined as institutional births, at the individual level. Women who had a pregnancy outcome (livebirth, stillbirth or abortion) 12 months prior to being surveyed were eligible for interview. Random effects logistic regression was used to evaluate the effect of the interventions.
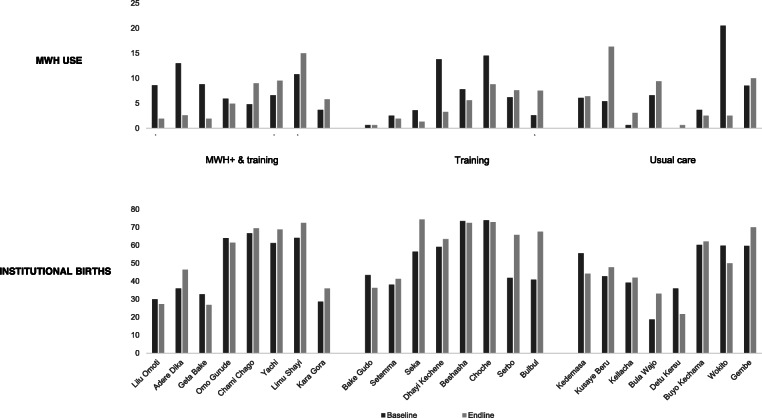
Data from 24 PHCUs and 7593 women were analysed using intention-to-treat. The proportion of institutional births was comparable at baseline between the three arms. At endline, institutional births were slightly higher in the MWH + training (54% [n = 671/1239]) and training only arms (65% [n = 821/1263]) compared to usual care (51% [n = 646/1271]). MWH use at baseline was 6.7% (n = 256/3784) and 5.8% at endline (n = 219/3809). Both intervention groups exhibited a non-statistically significant higher odds of institutional births compared to usual care (MWH & leader training odds ratio [OR] = 1.09, 97.5% confidence interval [CI] 0.67 to 1.75; leader training OR = 1.37, 97.5% CI 0.85 to 2.22).
Both the combined MWH & leader training and the leader training alone intervention led to a small but non-significant increase in institutional births when compared to usual care. Implementation challenges and short intervention duration may have hindered intervention effectiveness. Nevertheless, the observed increases suggest the interventions have potential to improve women's use of maternal healthcare services. Optimal distances at which MWHs are most beneficial to women need to be investigated.
The trial was retrospectively registered on the Clinical Trials website ( https://clinicaltrials.gov ) on 3rd October 2017. The trial identifier is NCT03299491 .
产妇候产之家(MWHs)是临近产科护理设施的供孕妇居住的场所,旨在消除获取医疗服务的身体障碍。然而,其效果尚未得到严格评估。这项整群随机试验的目的是评估功能性产妇候产之家与经过培训的当地领导人进行社区动员相结合,对改善埃塞俄比亚吉马地区机构分娩的效果。
在三个地区进行了一项实用的平行组整群随机试验。24个初级卫生保健单位(PHCUs)被随机分配到以下三组之一:(i)升级后的产妇候产之家并结合关于安全孕产策略的当地领导人培训;(ii)仅进行当地领导人培训;(iii)常规护理。在基线和干预后21个月通过重复横断面调查收集数据,以在个体层面评估干预对主要结局(定义为机构分娩)的影响。在接受调查前12个月有妊娠结局(活产、死产或流产)的妇女有资格接受访谈。采用随机效应逻辑回归来评估干预效果。
采用意向性分析对来自24个初级卫生保健单位和7593名妇女的数据进行了分析。三组在基线时机构分娩的比例相当。在终末评估时,与常规护理组(51% [n = 646/1271])相比,产妇候产之家 + 培训组(54% [n = 671/1239])和仅培训组(65% [n = 821/1263])的机构分娩比例略高。基线时产妇候产之家的使用率为6.7%(n = 256/3784),终末评估时为5.8%(n = 219/3809)。与常规护理相比,两个干预组的机构分娩几率均有非统计学意义的升高(产妇候产之家与领导人培训的优势比 [OR] = 1.09,97.5%置信区间 [CI] 0.67至1.75;领导人培训OR = 1.37,97.5% CI 0.85至2.22)。
与常规护理相比,产妇候产之家与领导人培训相结合以及仅进行领导人培训的干预措施均使机构分娩略有增加,但无统计学意义。实施方面的挑战和干预持续时间较短可能阻碍了干预效果。尽管如此,观察到的增加表明这些干预措施有潜力改善妇女对孕产妇医疗服务的利用。需要研究产妇候产之家对妇女最有益的最佳距离。
该试验于2017年10月3日在临床试验网站(https://clinicaltrials.gov)进行了回顾性注册。试验标识符为NCT03299491。