Scott Nancy A, Kaiser Jeanette L, Ngoma Thandiwe, McGlasson Kathleen L, Henry Elizabeth G, Munro-Kramer Michelle L, Biemba Godfrey, Bwalya Misheck, Sakanga Viviane R, Musonda Gertrude, Hamer Davidson H, Boyd Carol J, Bonawitz Rachael, Vian Taryn, Kruk Margaret E, Fong Rachel M, Chastain Parker S, Mataka Kaluba, Ahmed Mdluli Eden, Veliz Philip, Lori Jody R, Rockers Peter C
Department of Global Health, Boston University School of Public Health, Boston, Massachusetts, USA
Department of Global Health, Boston University School of Public Health, Boston, Massachusetts, USA.
BMJ Glob Health. 2021 Dec;6(12). doi: 10.1136/bmjgh-2021-006385.
Maternity waiting homes (MWHs) aim to increase access to maternity and emergency obstetric care by allowing women to stay near a health centre before delivery. An improved MWH model was developed with community input and included infrastructure, policies and linkages to health centres. We hypothesised this MWH model would increase health facility delivery among remote-living women in Zambia.
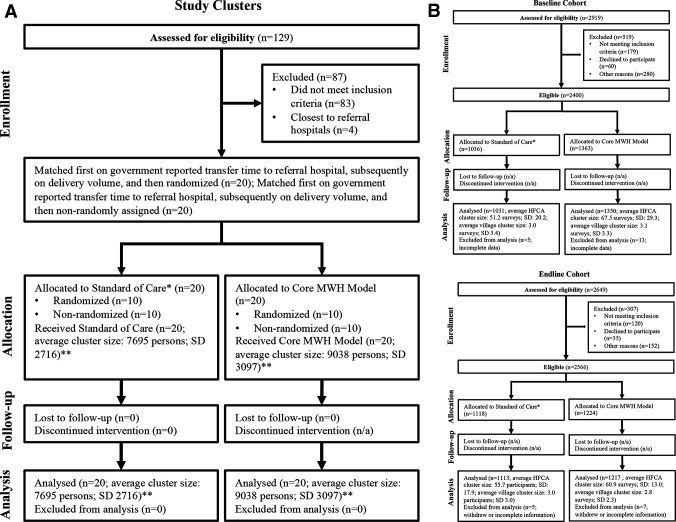
We conducted a quasi-experimental study at 40 rural health centres (RHC) that offer basic emergency obstetric care and had no recent stockouts of oxytocin or magnesium sulfate, located within 2 hours of a referral hospital. Intervention clusters (n=20) received an improved MWH model. Control clusters (n=20) implemented standard of care. Clusters were assigned to study arm using a matched-pair randomisation procedure (n=20) or non-randomly with matching criteria (n=20). We interviewed repeated cross-sectional random samples of women in villages 10+ kilometres from their RHC. The primary outcome was facility delivery; secondary outcomes included postnatal care utilisation, counselling, services received and expenditures. Intention-to-treat analysis was conducted. Generalised estimating equations were used to estimate ORs.
We interviewed 2381 women at baseline (March 2016) and 2330 at endline (October 2018). The improved MWH model was associated with increased odds of facility delivery (OR 1.60 (95% CI: 1.13 to 2.27); p<0.001) and MWH utilisation (OR 2.44 (1.62 to 3.67); p<0.001). The intervention was also associated with increased odds of postnatal attendance (OR 1.55 (1.10 to 2.19); p<0.001); counselling for family planning (OR 1.48 (1.15 to 1.91); p=0.002), breast feeding (OR 1.51 (1.20 to 1.90); p<0.001), and kangaroo care (OR 1.44 (1.15, 1.79); p=0.001); and caesarean section (OR 1.71 (1.16 to 2.54); p=0.007). No differences were observed in household expenditures for delivery.
MWHs near well-equipped RHCs increased access to facility delivery, encouraged use of facilities with emergency care capacity, and improved exposure to counselling. MWHs can be useful in the effort to increase delivery at advanced facilities in areas where substantial numbers of women live remotely.
NCT02620436.
产妇候产之家(MWHs)旨在通过让妇女在分娩前住在医疗中心附近,增加获得产科和紧急产科护理的机会。在社区参与下开发了一种改进的MWH模式,包括基础设施、政策以及与医疗中心的联系。我们假设这种MWH模式将增加赞比亚偏远地区妇女在医疗机构分娩的比例。
我们在40个农村医疗中心(RHC)进行了一项准实验研究,这些中心提供基本的紧急产科护理,且催产素或硫酸镁近期无缺货情况,距离转诊医院在2小时路程内。干预组(n = 20)采用改进的MWH模式。对照组(n = 20)实施常规护理。通过配对随机化程序(n = 20)或根据匹配标准非随机地将组分配到研究组(n = 20)。我们对距离其RHC 10公里以上村庄的妇女进行了重复横断面随机抽样访谈。主要结局是在医疗机构分娩;次要结局包括产后护理利用情况、咨询、接受的服务和支出。进行意向性分析。使用广义估计方程来估计比值比(OR)。
我们在基线(2016年3月)访谈了2381名妇女,在随访结束(2018年10月)时访谈了2330名妇女。改进的MWH模式与在医疗机构分娩的几率增加相关(OR 1.60(95%可信区间:1.13至2.27);p<0.001)以及MWH的利用率增加(OR 2.44(1.62至3.67);p<0.001)。该干预还与产后就诊几率增加相关(OR 1.55(1.10至2.19);p<0.001);计划生育咨询(OR 1.48(1.15至1.91);p = 0.002)、母乳喂养(OR 1.51(1.20至1.90);p<0.001)以及袋鼠式护理(OR 1.44(1.15,1.79);p = 0.001);还有剖宫产(OR 1.71(1.16至2.54);p = 0.007)。在分娩的家庭支出方面未观察到差异。
设备完善的RHC附近的MWHs增加了在医疗机构分娩的机会,鼓励使用具备紧急护理能力的设施,并改善了咨询服务的可及性。在大量妇女居住偏远的地区,MWHs有助于增加在高级设施分娩的比例。
NCT02620436。