School of Life Sciences and the State Key Laboratory of Pharmaceutical Biotechnology, Nanjing University, Nanjing, China.
National Health Commission Key Laboratory of Parasitic Disease Control and Prevention, Jiangsu Provincial Key Laboratory on Parasite and Vector Control Technology, Jiangsu Institute of Parasitic Diseases, Wuxi, China.
Front Immunol. 2020 Oct 7;11:570524. doi: 10.3389/fimmu.2020.570524. eCollection 2020.
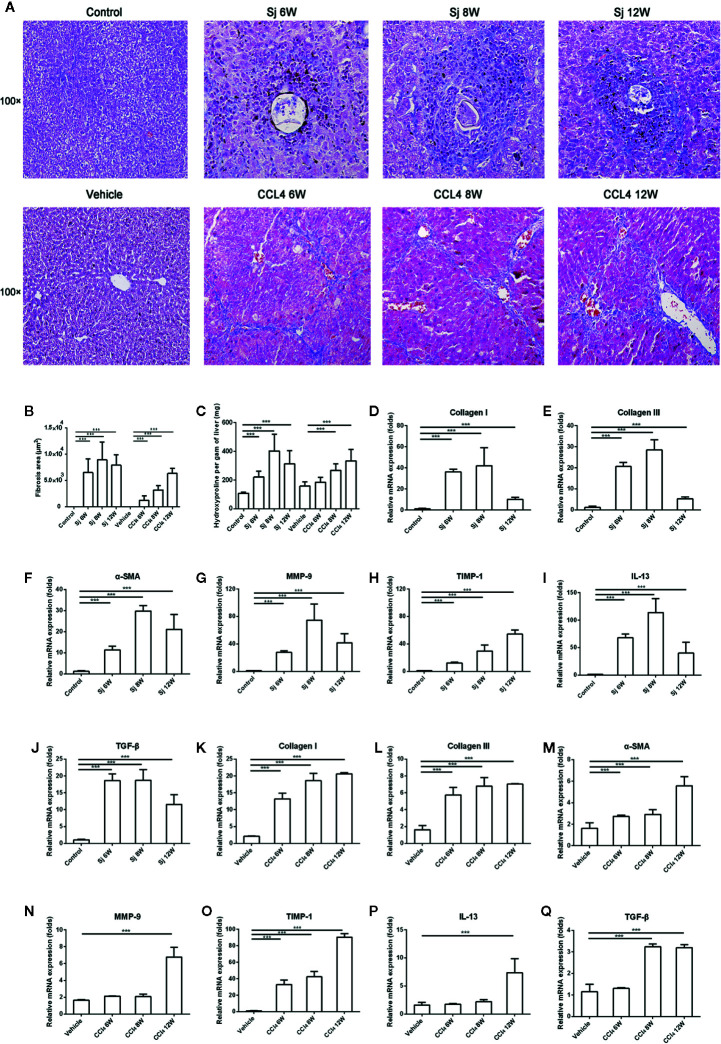
Liver fibrosis can result from various causes and could progress to cirrhosis and cancer; however, there are no effective treatments due to that its molecular mechanism is unclear. liver fibrosis model made by () infection or Carbon tetrachloride (CCl) intraperitoneal injection is a conventional model used in liver fibrosis-related studies for mechanism or pharmaceutical research purposes. But the differences in the pathological progression, immune responses and the underlying mechanism between the two liver fibrosis model have not been carefully compared and characterized, which hinders us from correctly understanding and making better use of the two models. In the present study, the pathological changes to the liver, and the cytokines, inflammatory factors, macrophages, and lymphocytes subsets involved were analyzed in the liver fibrosis model of infection or CCl intraperitoneal injection. Additionally, the pathological progression, immune responses and the underlying injury mechanism in these two models were compared and characterized. The results showed that the changing trend of interleukin-13 (IL-13), transforming growth factor beta (TGF-β), inflammatory factors, and M1, M2 macrophages, were consistent with the development trend of fibrosis regardless of whether liver fibrosis was caused by or CCl. For lymphocyte subsets, the proportions of CD3 T cells and CD4 T cells decreased gradually, while proportion of CD8 T cells peaked at 6 weeks in mice infected with and at 12 weeks in mice injected with CCl. With prolonged . infection time, Th1 (CD4IFN-γ) immunity converted to Th2 (CD4IL-4)/Th17 (CD4IL-17) with weaker regulatory T cell (Treg) (CD4CD25FOXP3) immunity. However, in liver fibrosis caused by CCl, Th1 cells occupied the dominant position, while proportions of Th2, Th17, and Treg cells decreased gradually. In conclusion, liver fibrosis was a complex pathological process that was regulated by a series of cytokines and immune cells. The pathological progressions and immune responses to or CCl induced liver fibrosis were different, possibly because of their different injury mechanisms. The appropriate animal model should be selected according to the needs of different experiments and the pathogenic factors of liver fibrosis in the study.
肝纤维化可由多种原因引起,并可能进展为肝硬化和肝癌;然而,由于其分子机制尚不清楚,因此尚无有效的治疗方法。 () 感染或四氯化碳 (CCl) 腹腔注射引起的肝纤维化模型是肝纤维化相关研究中用于机制或药物研究目的的常规模型。但是,这两种肝纤维化模型的病理进展、免疫反应和潜在机制之间的差异尚未得到仔细比较和表征,这阻碍了我们正确理解和更好地利用这两种模型。在本研究中,分析了 () 感染或 CCl 腹腔注射引起的肝纤维化模型中肝的病理变化以及涉及的细胞因子、炎症因子、巨噬细胞和淋巴细胞亚群。此外,比较和表征了这两种模型的病理进展、免疫反应和潜在损伤机制。结果表明,白细胞介素-13 (IL-13)、转化生长因子-β (TGF-β)、炎症因子和 M1、M2 巨噬细胞的变化趋势与纤维化的发展趋势一致,无论肝纤维化是由 还是 CCl 引起的。对于淋巴细胞亚群,CD3 T 细胞和 CD4 T 细胞的比例逐渐下降,而 CD8 T 细胞的比例在感染的小鼠中在 6 周时达到峰值,在注射 CCl 的小鼠中在 12 周时达到峰值。随着感染时间的延长,Th1 (CD4IFN-γ) 免疫向 Th2 (CD4IL-4)/Th17 (CD4IL-17) 转化,调节性 T 细胞 (Treg) (CD4CD25FOXP3) 免疫减弱。然而,在 CCl 引起的肝纤维化中,Th1 细胞占据主导地位,而 Th2、Th17 和 Treg 细胞的比例逐渐下降。总之,肝纤维化是一个复杂的病理过程,受一系列细胞因子和免疫细胞的调节。 () 或 CCl 诱导的肝纤维化的病理进展和免疫反应不同,可能是由于它们不同的损伤机制。应根据不同实验的需要和研究中肝纤维化的致病因素选择合适的动物模型。