Amri Parviz, Nikbakhsh Novin, Modaress Seyed Reza, Nosrati Ramin
Clinical Research Development Unit of Rouhani Hospital, Babol University of Medical Sciences, Babol, Iran.
Anesth Pain Med. 2020 Jul 6;10(4):e99796. doi: 10.5812/aapm.99796. eCollection 2020 Aug.
Rigid bronchoscopy is often used to diagnose and treat the location of resection of the tracheal stenosis. It is a selective procedure for the dilatation of tracheal stenosis, especially when accompanied by respiratory distress.
We introduced patients who were diagnosed with tracheal stenosis and candidate for rigid bronchoscopy dilatation by the upper airway nerve blocks.
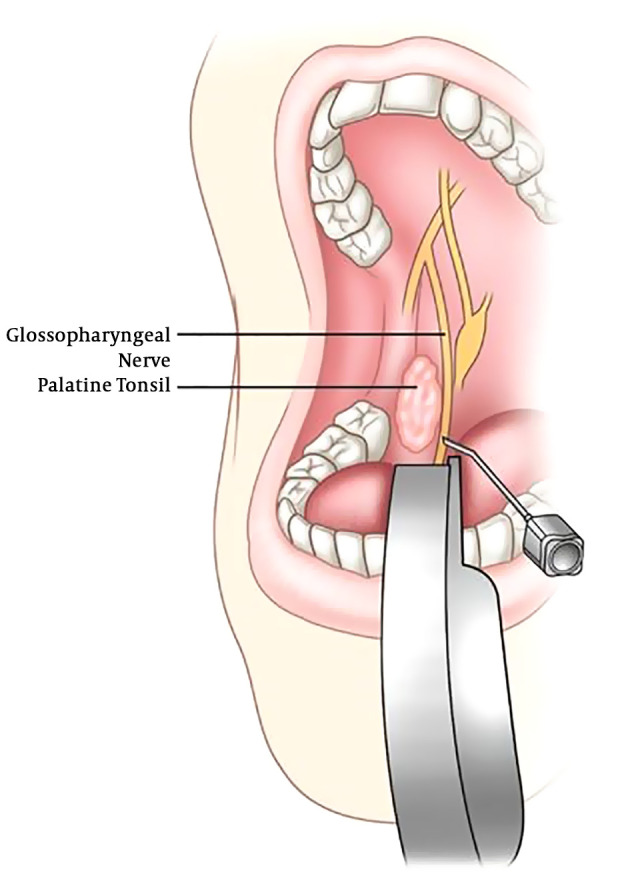
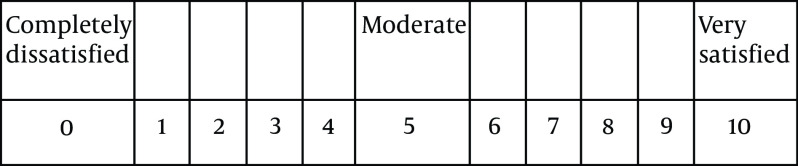
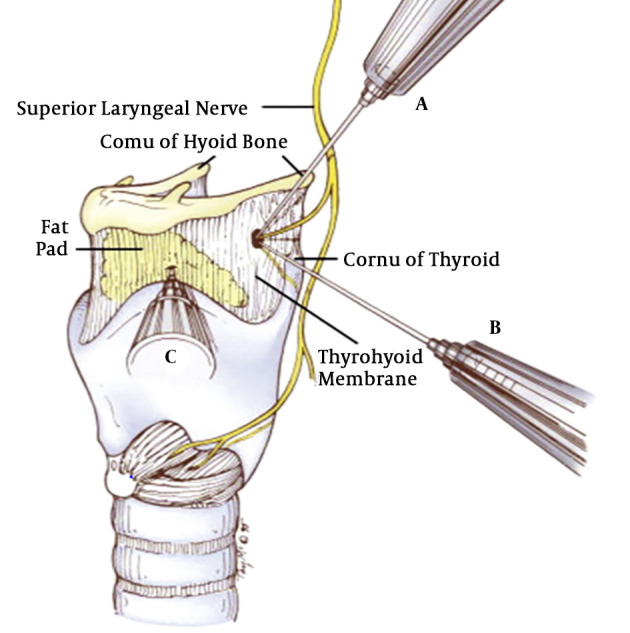
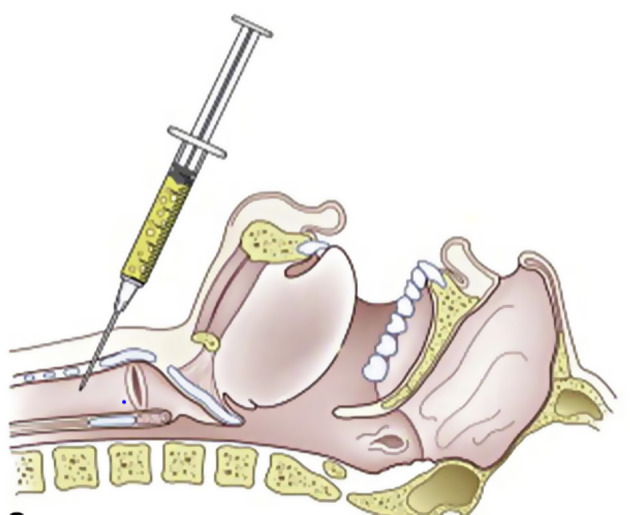
This prospective observational study was conducted on 17 patients who underwent dilatation with rigid bronchoscopy in tracheal stenosis at Hospitals affiliated with Babol University of Medical Sciences from 2002 to 2017. The patients were given three nerve blocks, 6 bilateral superior laryngeal nerve block, bilateral glossopharyngeal nerve block, and recurrent laryngeal nerve block (transtracheal) before awake rigid bronchoscopy using 2% lidocaine. We evaluated the demographic data, the cause of tracheal stenosis, the quality of the airway nerve block (Intubation score), patients' satisfaction from bronchoscopy and thoracic surgeons' satisfaction. Complications of nerve blocks were recorded.
From 2002 to 2017, 17 patients (14 were male and 3 were) female with tracheal stenosis who were candidates for dilatation with bronchoscopy and accepted the upper nerve block were included. The quality of the block was acceptable in 16 (94%) patients. 15 patients received fentanyl, and only two patients did not need to intravenous sedation. The mean age of patients was 29.59 ± 11.59. The average satisfaction of the surgeon was 8.82 ± 1.13 and the satisfaction of patients with anesthesia was 8.89 ± 1.16. There was one serious complication (laryngospasm) in one patient.
The upper airway nerve block method is a suitable anesthesia technique for patients with tracheal stenosis who are candidates for the tracheal dilatation with rigid bronoscopy, especially when the patient has respiratory distress and has not been evaluated before surgery.
硬质支气管镜常用于诊断和治疗气管狭窄的切除部位。对于气管狭窄的扩张,尤其是伴有呼吸窘迫时,它是一种选择性手术。
我们介绍了经上气道神经阻滞诊断为气管狭窄并适合进行硬质支气管镜扩张的患者。
这项前瞻性观察性研究对2002年至2017年在巴博尔医科大学附属医院接受气管狭窄硬质支气管镜扩张的17例患者进行。在清醒硬质支气管镜检查前,使用2%利多卡因对患者进行三次神经阻滞,即6次双侧喉上神经阻滞、双侧舌咽神经阻滞和喉返神经阻滞(经气管)。我们评估了人口统计学数据、气管狭窄的原因、气道神经阻滞的质量(插管评分)、患者对支气管镜检查的满意度以及胸外科医生的满意度。记录神经阻滞的并发症。
2002年至2017年,纳入了17例气管狭窄患者(14例男性,3例女性),他们适合进行支气管镜扩张并接受了上神经阻滞。16例(94%)患者的阻滞质量可接受。15例患者接受了芬太尼,只有2例患者不需要静脉镇静。患者的平均年龄为29.59±11.59。外科医生的平均满意度为8.82±1.13,患者对麻醉的满意度为8.89±1.16。1例患者出现1例严重并发症(喉痉挛)。
上气道神经阻滞方法是适合气管狭窄且适合进行硬质支气管镜气管扩张的患者的麻醉技术,尤其是当患者有呼吸窘迫且术前未进行评估时。