Steendam Christi M J, Veerman G D Marijn, Pruis Melinda A, Atmodimedjo Peggy, Paats Marthe S, van der Leest Cor, von der Thüsen Jan H, Yick David C Y, Oomen-de Hoop Esther, Koolen Stijn L W, Dinjens Winand N M, van Schaik Ron H N, Mathijssen Ron H J, Aerts Joachim G J V, Dubbink Hendrikus Jan, Dingemans Anne-Marie C
Department of Pulmonology, Erasmus MC Cancer Institute, University Medical Center, 3015 GD Rotterdam, The Netherlands.
Department of Pulmonology, Amphia Hospital, 4818 CK Breda, The Netherlands.
Cancers (Basel). 2020 Oct 29;12(11):3179. doi: 10.3390/cancers12113179.
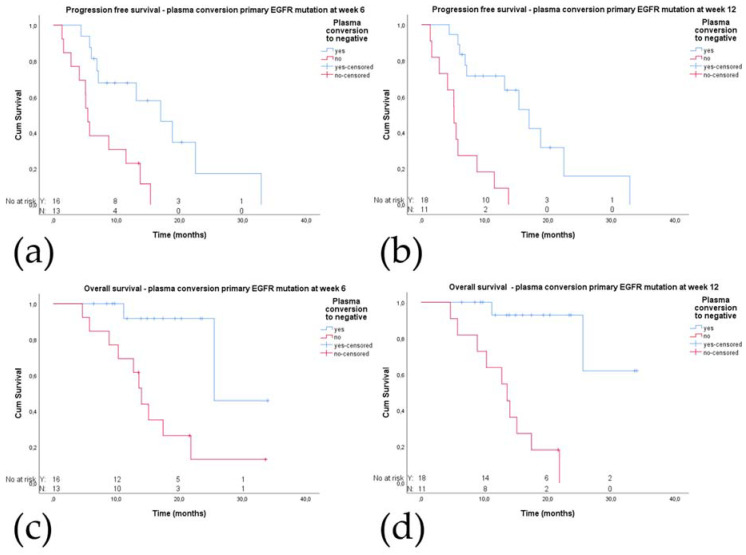
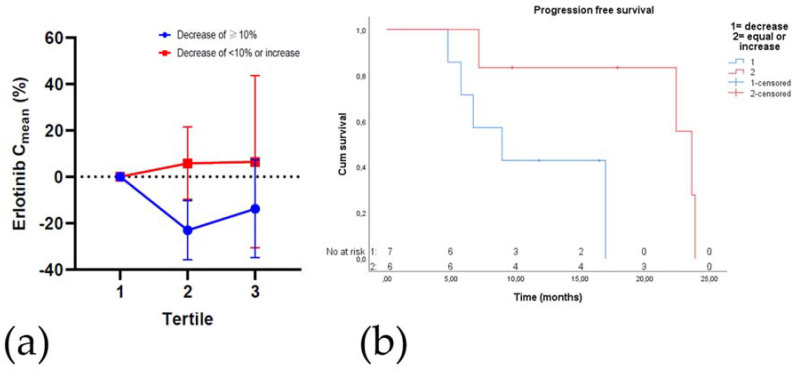
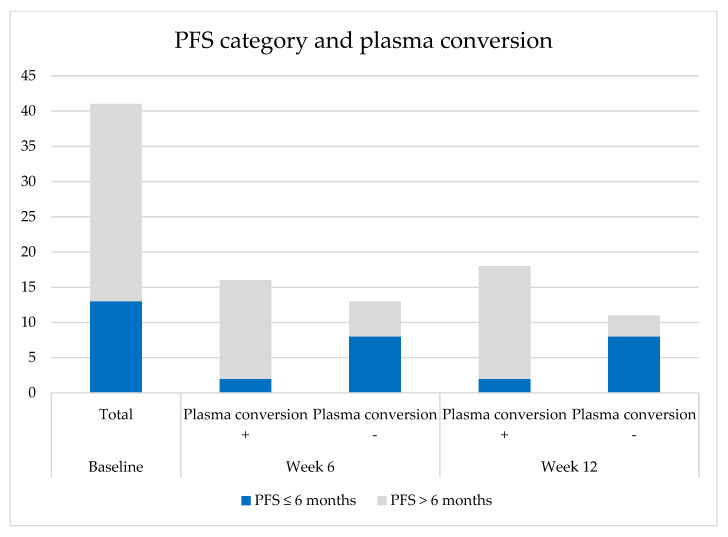
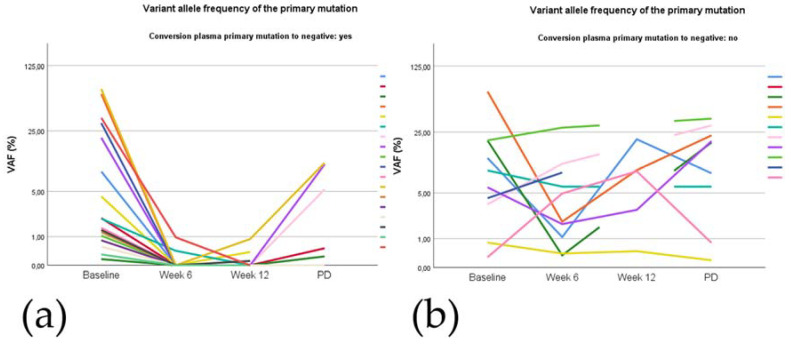
Although epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitors (TKIs) are the preferred treatment for patients with -mutated non-small cell lung cancer (NSCLC), not all patients benefit. We therefore explored the impact of the presence of mutations found in cell-free DNA (cfDNA) and TKI plasma concentrations during treatment on progression-free survival (PFS). In the prospective START-TKI study blood samples from 41 patients with -mutated NSCLC treated with EGFR-TKIs were available. Next generation sequencing (NGS) on cfDNA was performed, and plasma TKI concentrations were measured. Patients without complete plasma conversion of mutation at week 6 had a significantly shorter PFS (5.5 vs. 17.0 months, = 0.002) and OS (14.0 vs. 25.5 months, = 0.003) compared to patients with plasma conversion. In thirteen (second line) osimertinib-treated patients with a (plasma or tissue) concomitant mutation at baseline, PFS was significantly shorter compared to six wild-type cases; 8.8 vs. 18.8 months, = 0.017. Erlotinib C decrease of ≥10% in the second tertile of treatment was also associated with a significantly shorter PFS; 8.9 vs. 23.6 months, = 0.037. We obtained evidence that absence of plasma loss of the primary mutation, isolated plasma p.T790M loss after six weeks, baseline concomitant mutations, and erlotinib C decrease during treatment are probably related to worse outcome.
尽管表皮生长因子受体(EGFR)-酪氨酸激酶抑制剂(TKIs)是治疗表皮生长因子受体基因突变的非小细胞肺癌(NSCLC)患者的首选疗法,但并非所有患者都能从中获益。因此,我们探讨了游离DNA(cfDNA)中发现的突变以及治疗期间TKI血浆浓度对无进展生存期(PFS)的影响。在START-TKI前瞻性研究中,有41例接受EGFR-TKIs治疗的表皮生长因子受体基因突变的NSCLC患者的血样可供研究。对cfDNA进行了二代测序(NGS),并测量了血浆TKI浓度。与血浆转换的患者相比,在第6周时血浆中表皮生长因子受体基因突变未完全转换的患者的PFS(5.5个月对17.0个月,P=0.002)和总生存期(OS,14.0个月对25.5个月,P=0.003)明显更短。在13例(二线)接受奥希替尼治疗且基线时(血浆或组织)伴有表皮生长因子受体基因突变的患者中,与6例野生型患者相比,PFS明显更短;分别为8.8个月和18.8个月,P=0.017。在治疗的第二个三分位数中,厄洛替尼C降低≥10%也与明显更短的PFS相关;分别为8.9个月和23.6个月,P=0.037。我们获得的证据表明,原发性表皮生长因子受体基因突变的血浆未消失、六周后孤立的血浆p.T790M缺失、基线时伴有表皮生长因子受体基因突变以及治疗期间厄洛替尼C降低可能与较差的预后相关。