Department of Pharmaceutics and Center for Pharmaceutical Engineering and Sciences, School of Pharmacy, Virginia Commonwealth University, Richmond, Virginia 23298, United States.
Department of Pathology, School of Medicine, Virginia Commonwealth University, Richmond, Virginia 23298, United States.
Mol Pharm. 2020 Dec 7;17(12):4691-4703. doi: 10.1021/acs.molpharmaceut.0c00983. Epub 2020 Nov 10.
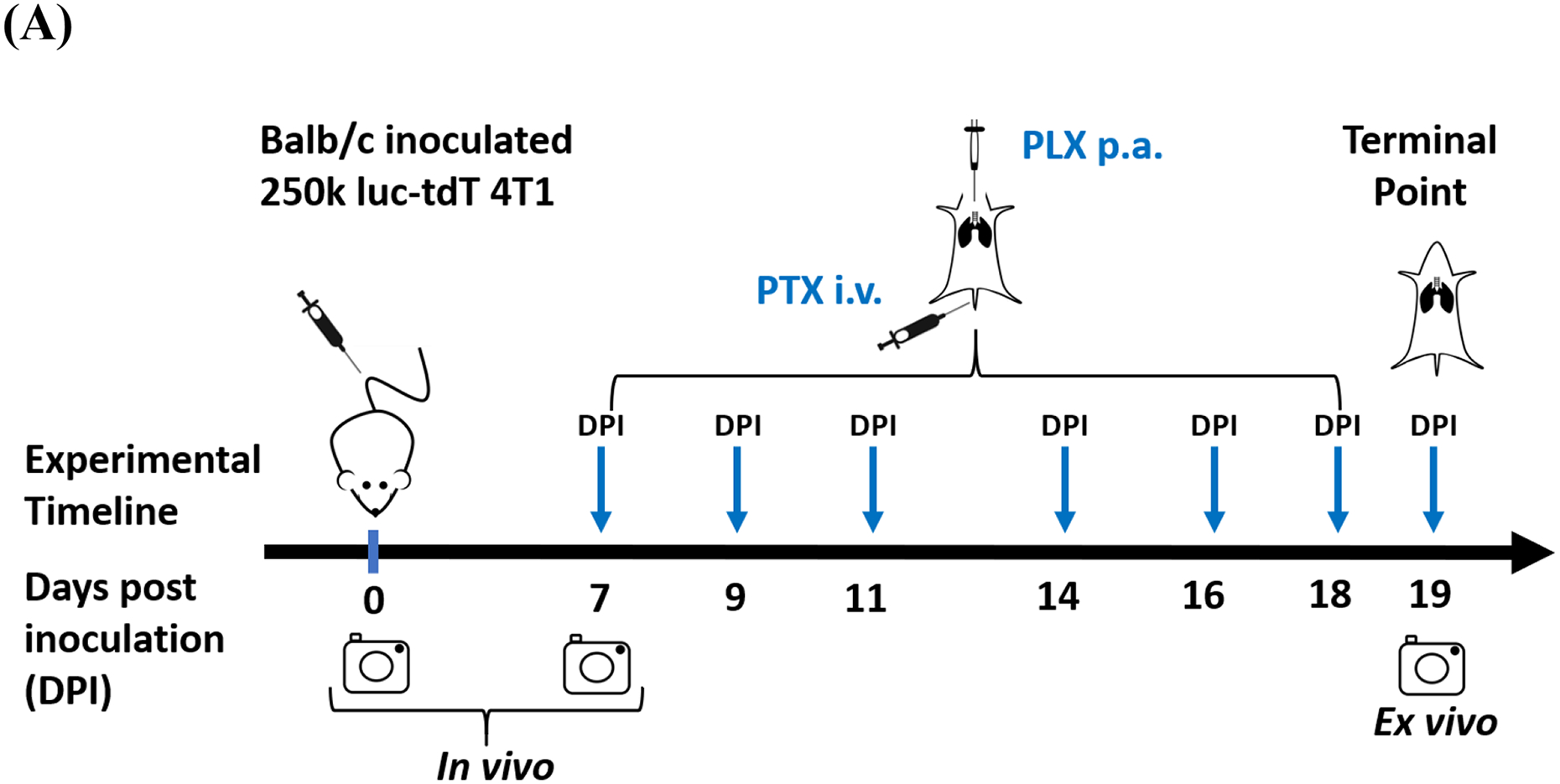
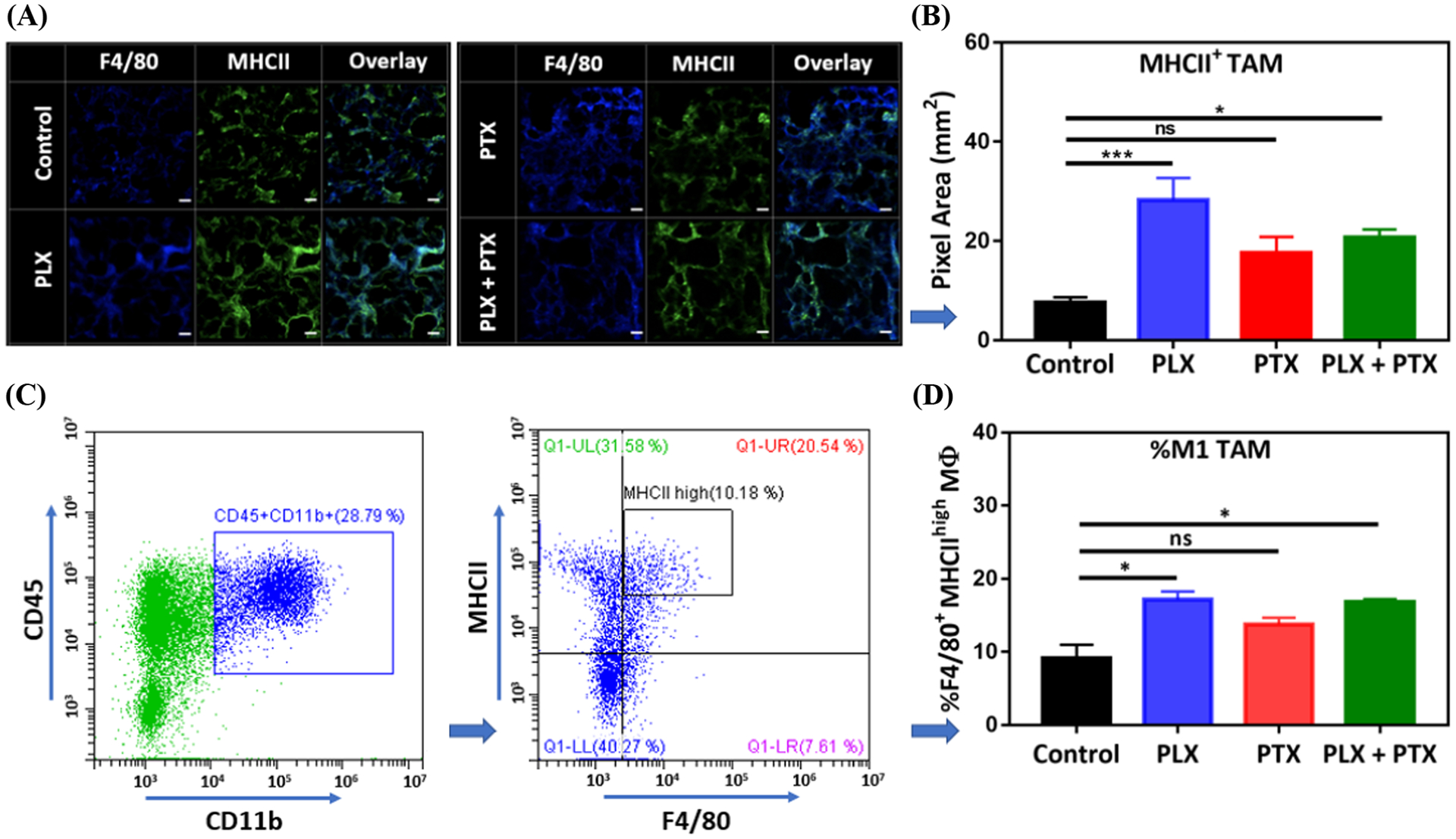
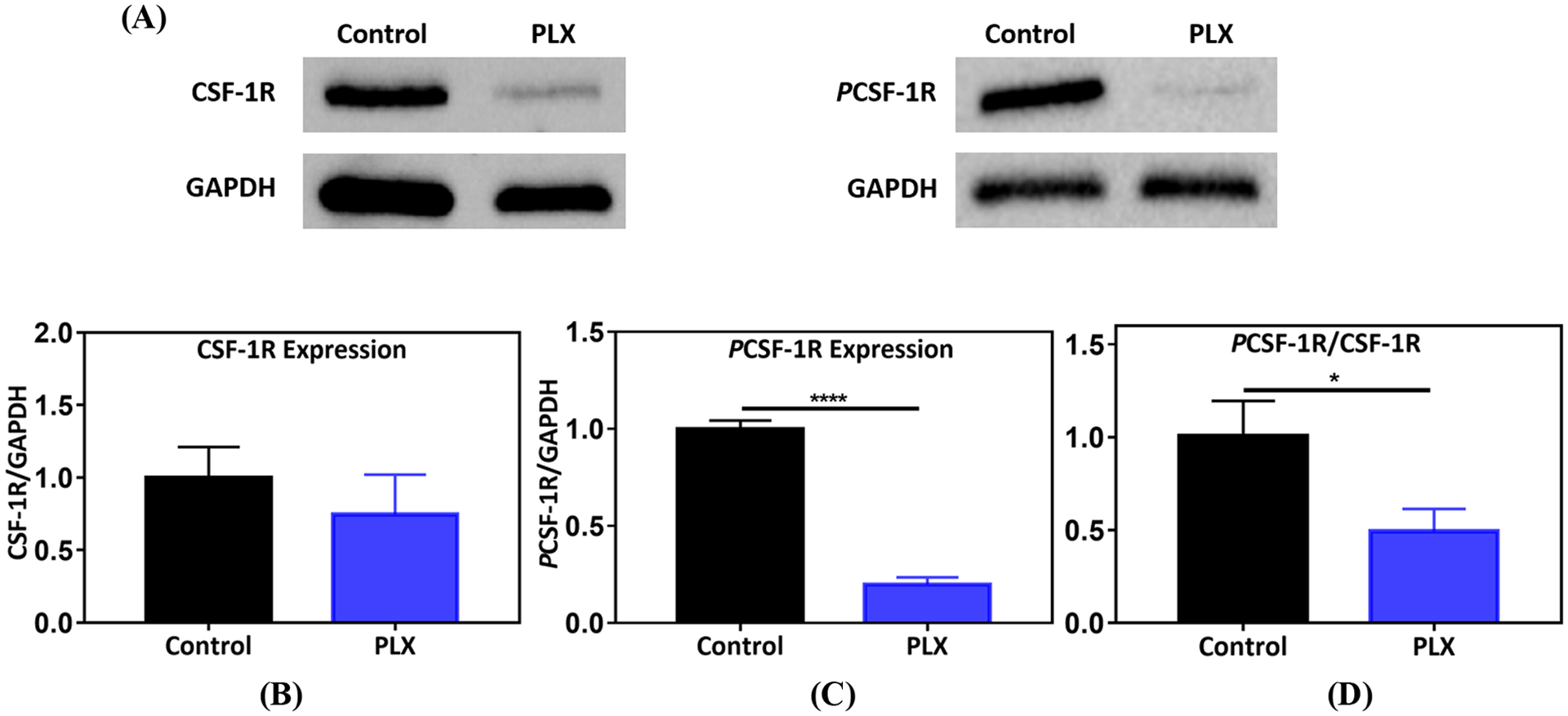
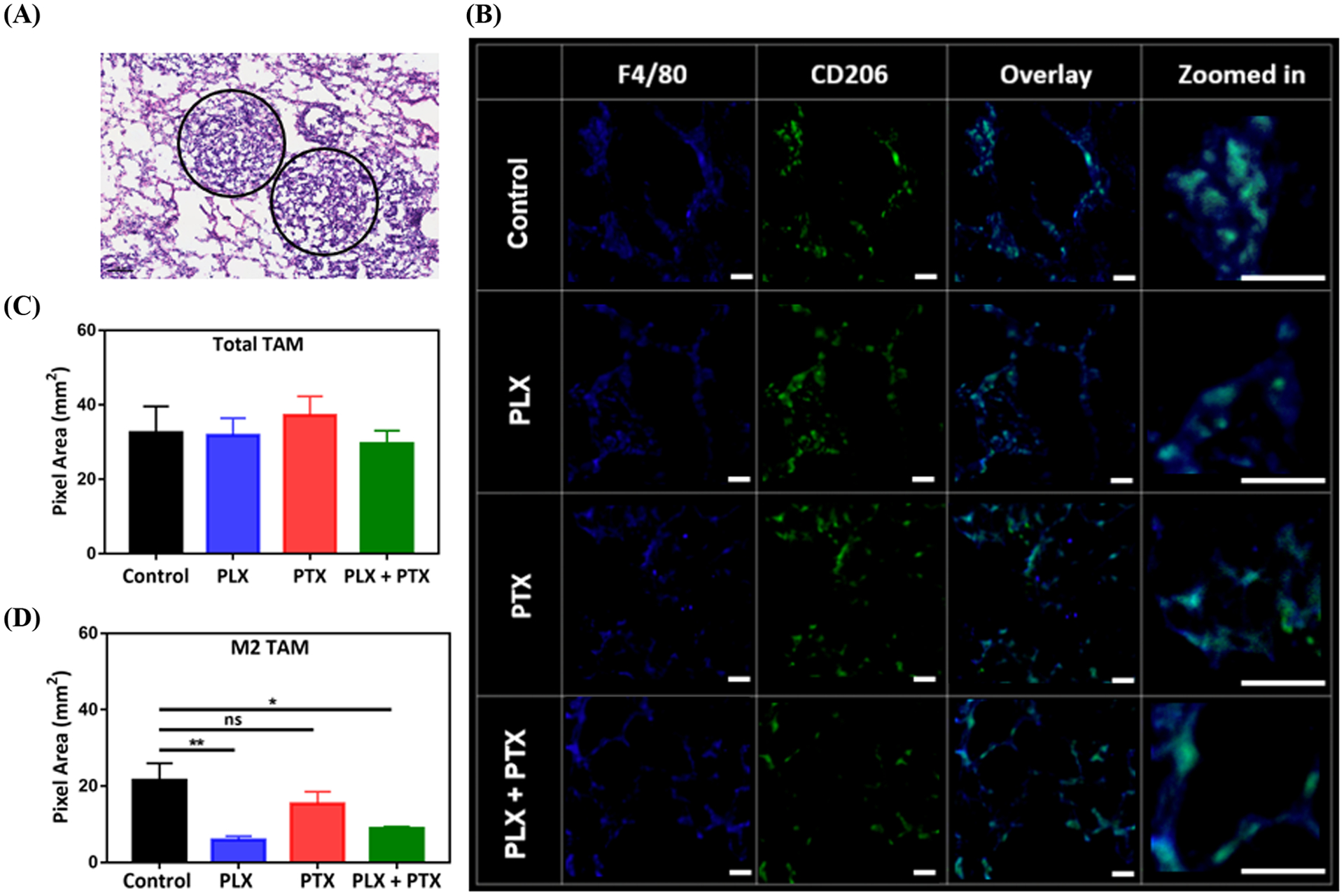
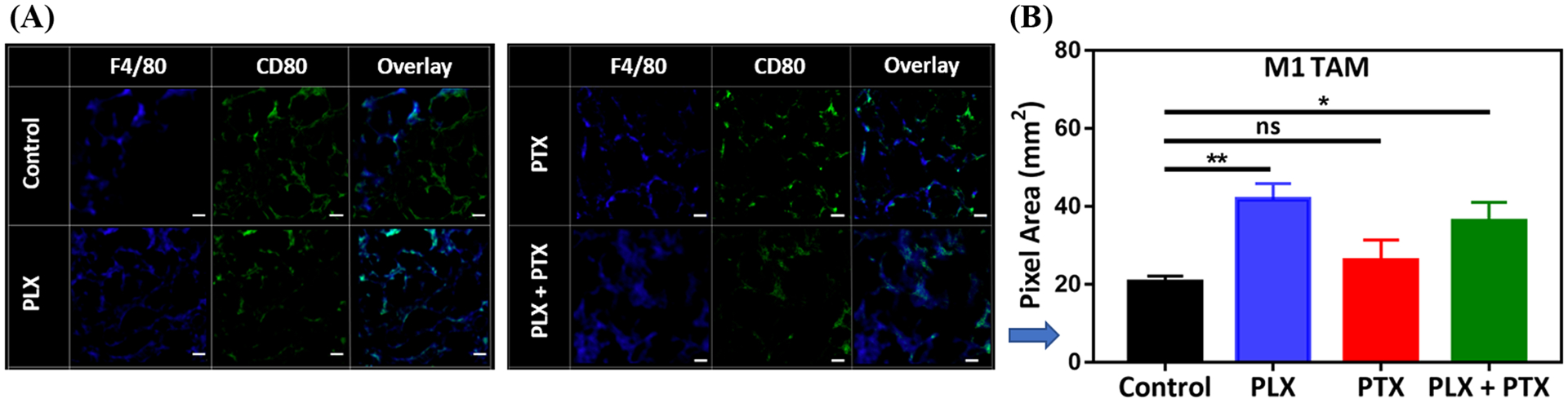
The lungs are major sites of metastases for several cancer types, including breast cancer (BC). Prognosis and quality of life of BC patients that develop pulmonary metastases are negatively impacted. The development of strategies to slow the growth and relieve the symptoms of BC lung metastases (BCLM) is thus an important goal in the management of BC. However, systemically administered first line small molecule chemotherapeutics have poor pharmacokinetic profiles and biodistribution to the lungs and significant off-target toxicity, severely compromising their effectiveness. In this work, we propose the local delivery of add-on immunotherapy to the lungs to support first line chemotherapy treatment of advanced BC. In a syngeneic murine model of BCLM, we show that local pulmonary administration (p.a.) of PLX-3397 (PLX), a colony-stimulating factor 1 receptor inhibitor (CSF-1Ri), is capable of overcoming physiological barriers of the lung epithelium, penetrating the tumor microenvironment (TME), and decreasing phosphorylation of CSF-1 receptors, as shown by the Western blot of lung tumor nodules. That inhibition is accompanied by an overall decrease in the abundance of protumorigenic (M2-like) macrophages in the TME, with a concomitant increase in the amount of antitumor (M1-like) macrophages when compared to the vehicle-treated control. These effects with PLX (p.a.) were achieved using a much smaller dose (1 mg/kg, every other day) compared to the systemic doses typically used in preclinical studies (40-800 mg/kg/day). As an additive in combination with intravenous (i.v.) administration of paclitaxel (PTX), PLX (p.a.) leads to a decrease in tumor burden without additional toxicity. These results suggested that the proposed immunochemotherapy, with regional pulmonary delivery of PLX along with the i.v. standard of care chemotherapy, may lead to new opportunities to improve treatment, quality of life, and survival of patients with BCLM.
肺部是包括乳腺癌(BC)在内的几种癌症类型转移的主要部位。发生肺转移的 BC 患者的预后和生活质量受到负面影响。因此,开发减缓 BC 肺转移(BCLM)生长和缓解症状的策略是 BC 管理的重要目标。然而,全身给予一线小分子化疗药物具有较差的药代动力学特征和肺部生物分布,以及显著的脱靶毒性,严重影响其疗效。在这项工作中,我们提出将附加免疫疗法局部递送至肺部,以支持晚期 BC 的一线化疗治疗。在 BCLM 的同源小鼠模型中,我们表明局部肺给药(p.a.)PLX-3397(PLX),一种集落刺激因子 1 受体抑制剂(CSF-1Ri),能够克服肺上皮的生理屏障,穿透肿瘤微环境(TME),并降低 CSF-1 受体的磷酸化,如肺肿瘤结节的 Western blot 所示。这种抑制伴随着 TME 中促肿瘤(M2 样)巨噬细胞丰度的整体减少,同时与载体处理对照相比,抗肿瘤(M1 样)巨噬细胞的数量增加。与临床前研究中通常使用的全身剂量(40-800mg/kg/天)相比,PLX(p.a.)实现了这些效果,使用的剂量要小得多(1mg/kg,隔天一次)。作为与静脉(i.v.)给予紫杉醇(PTX)联合的附加物,PLX(p.a.)导致肿瘤负担减少而没有额外的毒性。这些结果表明,局部肺递送达 PLX 与 i.v.标准护理化疗相结合的拟议免疫化疗可能为改善 BCLM 患者的治疗、生活质量和生存率提供新的机会。