Schuurmans Jaap, Crol Chantalle, Olde Rikkert Marcel, Engels Yvonne
GP, Radboud University, Groesbeek, The Netherlands
Researcher, Department of Anesthesiology, Pain and Palliative Medicine, Radboud University, Nijmegen, Netherlands.
BJGP Open. 2021 Feb 23;5(1). doi: 10.3399/bjgpopen20X101123. Print 2021 Jan.
In the Netherlands during the past decade, a growing number of people with dementia requested euthanasia, and each year more of such requests were granted.
To obtain quantitative insights into the problems and needs of GPs when confronted with a euthanasia request by a person with dementia.
DESIGN & SETTING: A concept survey was composed for GPs in the Netherlands. Expert validity of the survey was achieved through pilot testing.
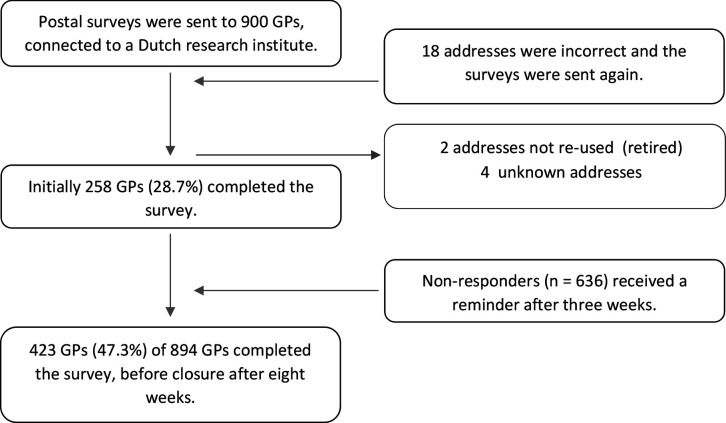
A postal survey was sent to a random sample of 900 Dutch GPs, regardless of their opinion on, or practical experience with, euthanasia. Collected data were analysed with descriptive statistics.
Of 894 GPs, 423 (47.3%) completed the survey, of whom 176 (41.6%) had experience with euthanasia requests from people with dementia. Emotional burden was reported most frequently ( = 86; 52.8%), as well as feeling uncertain about the mental competence of the person with dementia ( = 77; 47.2%), pressure by relatives ( = 70; 42.9%) or the person with dementia ( = 56; 34.4%), and uncertainty about handling advance euthanasia directives (AEDs) ( = 43; 26.4%). GPs would appreciate more support from the following: a support and consultation in euthanasia in the Netherlands (SCEN) physician (an independent physician for support, information, and formal consultation around euthanasia) ( = 291; 68. 8%); a geriatric consultation team ( = 185; 43.7%); the end-of-life clinic ( = 184; 43.5%); or a palliative care consultation team ( = 179; 42.3%). Surprisingly the need for moral deliberation was hardly mentioned.
The reported burden and the rise in numbers and complexity of euthanasia requests from people with dementia warrants primary care support. There needs to be easier access to colleagues with expertise, and training on end-of-life care needs of patients with dementia and their caregivers.
在过去十年间,荷兰越来越多的痴呆症患者请求安乐死,且每年获批的此类请求数量都在增加。
深入了解全科医生在面对痴呆症患者的安乐死请求时所面临的问题和需求。
为荷兰的全科医生设计了一项概念性调查。通过预试验确保了调查的专家效度。
向900名荷兰全科医生的随机样本邮寄调查问卷,无论他们对安乐死的看法或实际经验如何。收集的数据采用描述性统计进行分析。
894名全科医生中,423名(47.3%)完成了调查,其中176名(41.6%)有处理痴呆症患者安乐死请求的经验。报告最多的是情感负担(n = 86;52.8%),以及对痴呆症患者精神能力的不确定感(n = 77;47.2%)、亲属(n = 70;42.9%)或痴呆症患者本人(n = 56;34.4%)施加的压力,以及对处理生前预嘱(AEDs)的不确定感(n = 43;26.4%)。全科医生希望得到以下方面更多的支持:荷兰安乐死支持与咨询(SCEN)医生(一名围绕安乐死提供支持、信息和正式咨询的独立医生)(n = 291;68.8%);老年病咨询团队(n = 185;43.7%);临终关怀诊所(n = 184;43.5%);或姑息治疗咨询团队(n = 179;42.3%)。令人惊讶的是,几乎没有人提到需要进行道德审议。
所报告的负担以及痴呆症患者安乐死请求数量的增加和复杂性,表明需要初级保健支持。需要更容易获得具有专业知识的同事的帮助,以及针对痴呆症患者及其护理人员临终关怀需求的培训。