Division of Gastroenterology and Hepatology, Stanford University Medical Center, Palo Alto, California.
Asian Liver Center, Stanford University School of Medicine, Stanford, California.
JAMA Netw Open. 2020 Nov 2;3(11):e2022388. doi: 10.1001/jamanetworkopen.2020.22388.
The World Health Assembly has called for the elimination of hepatitis B and C by 2030. As hepatitis B has no cure, the US strategy to eliminate hepatitis B has focused on prevention through vaccination. However, there are limited data on the trend in vaccine-associated immunity since the US implementation of universal infant hepatitis B vaccination.
To compare self-reported hepatitis B vaccination coverage among children and adolescents with serologic evidence of immunity and infection in the US from 1999 to 2016.
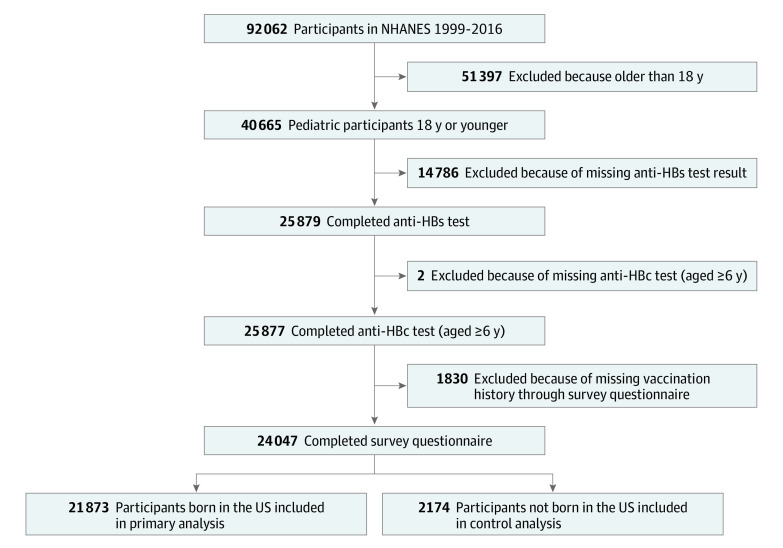
DESIGN, SETTING, AND PARTICIPANTS: This population-based cross-sectional study used data from the National Health and Nutrition Examination Survey (NHANES) from 1999 to 2016. US-born persons aged 2 to 18 years without missing hepatitis B serologic test results and with reported vaccination history were included. Data were analyzed from September 2017 to June 2018.
The proportion of participants who reported complete vaccination for hepatitis B and who had positive serologic test results indicating immunity.
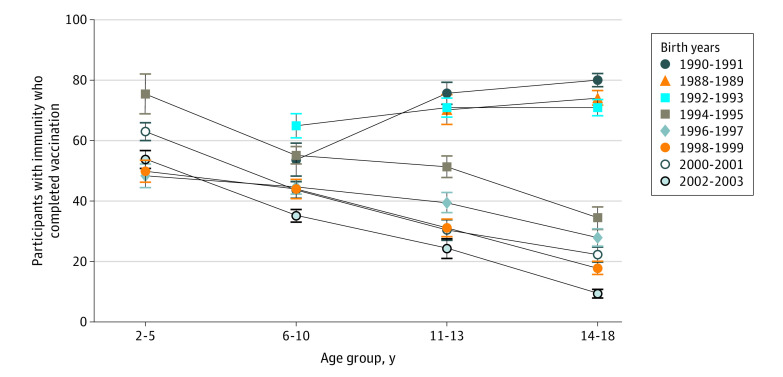
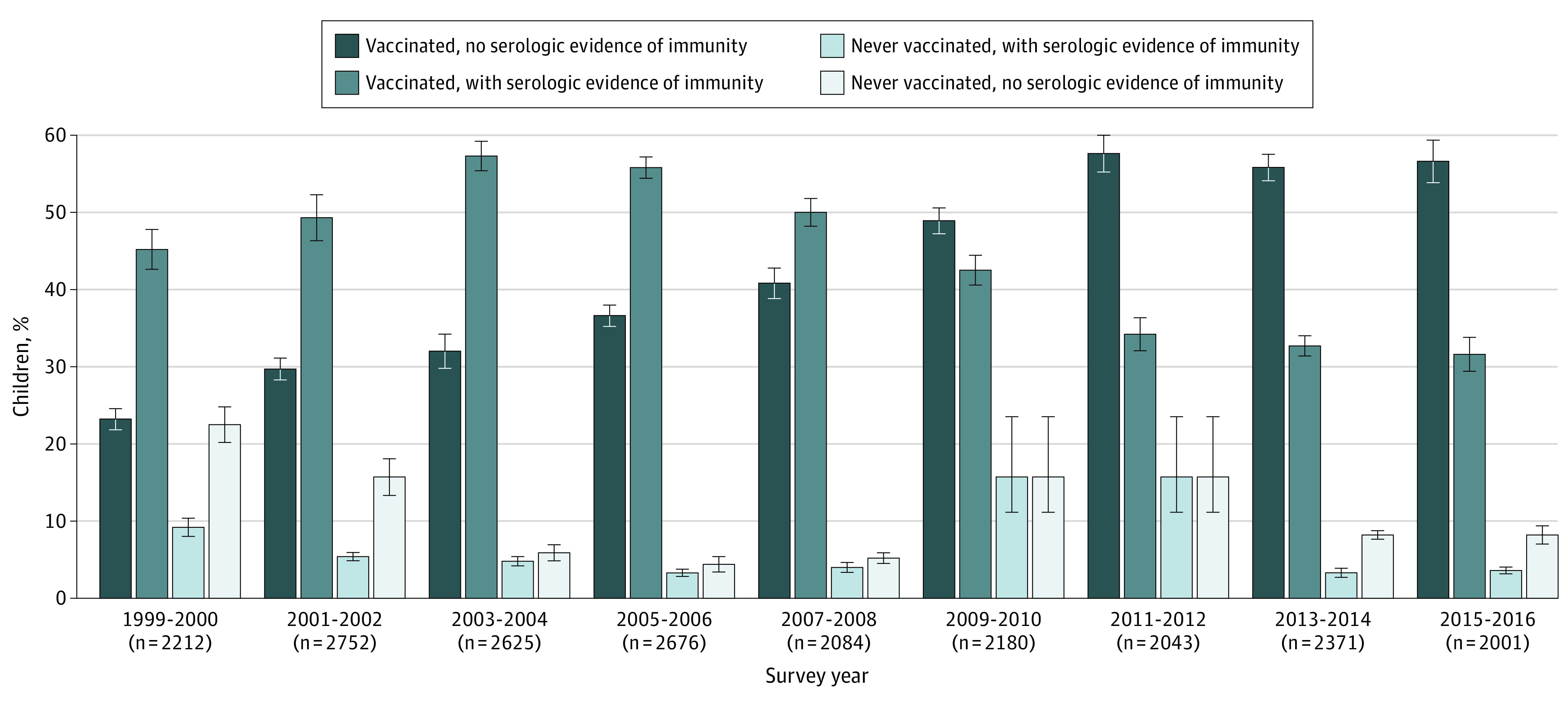
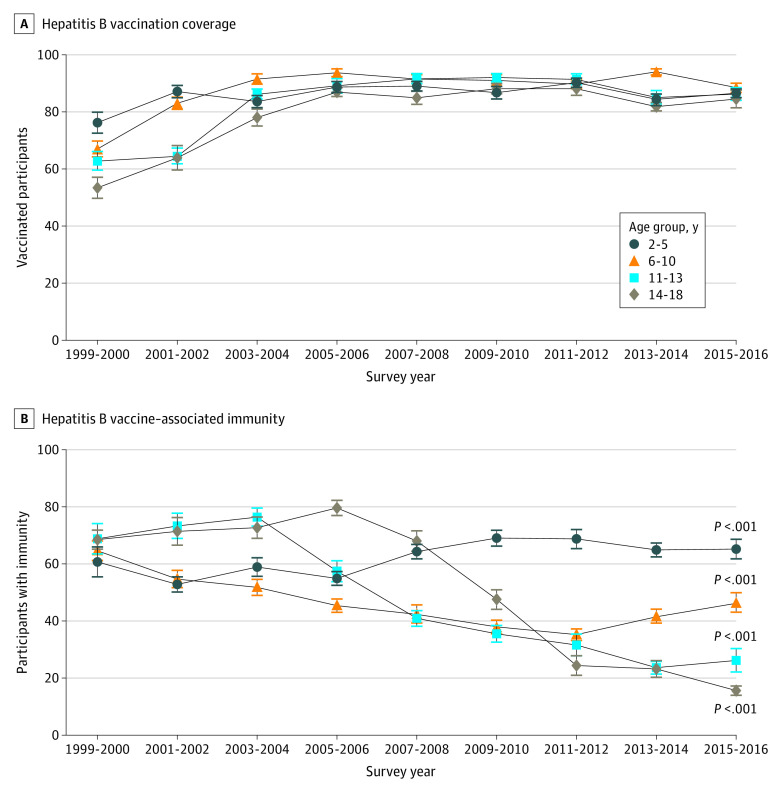
Of 21 873 children and adolescents, 51.2%% were male, and the mean (SD) age was 10.6 (4.6) years. The survey reported that hepatitis B vaccination coverage increased significantly from 1999 to 2016 (from 62.6% [95% CI, 58.6%-66.4%] to 86.3% [95% CI, 82.9%-89.2%]; P < .001). Vaccine-associated immunity also increased from 1999 to 2016 among children aged 2 to 5 years (from 60.7% [95% CI, 48.8%-71.4%] to 65.2% [95% CI, 57.4%-72.3%]; P = .001) but decreased among children aged 6 to 10 years (from 64.6% [95% CI, 57.7%-70.9%] to 46.5% [95% CI, 39.1%-54.0%]; P < .001), adolescents aged 11 to 13 years (from 68.8% [95% CI, 58.1%-77.8%] to 26.2% [95% CI, 18.6%-35.5%]; P < .001), and adolescents aged 14 to 18 years (from 68.5% [95% CI, 62.9%-73.6%] to 15.6% [95% CI, 12.2%-19.8%]; P < .001). By birth year, serologic evidence of vaccine-associated immunity significantly decreased in the 1994-2003 NHANES birth cohort but not among those born between 1988 and 1993. Non-US-born children and adolescents did not show the same decreasing trend in immunity.
In this cross-sectional study, decreasing hepatitis B immunity was observed among US-born children and adolescents in the 1994-2003 NHANES birth cohort despite increasing rates of hepatitis B vaccination coverage. These findings suggest a possible need for surveillance and a booster vaccine dose for hepatitis B as those without serologic evidence of immunity become young adults and may engage in behaviors associated with an increased risk for infection.
世界卫生大会呼吁到 2030 年消除乙型和丙型肝炎。由于乙型肝炎没有治愈方法,美国消除乙型肝炎的策略侧重于通过疫苗接种进行预防。然而,自美国实施普遍婴儿乙型肝炎疫苗接种以来,关于疫苗相关免疫趋势的数据有限。
比较美国 1999 年至 2016 年儿童和青少年中自我报告的乙型肝炎疫苗接种率与血清学免疫和感染证据。
设计、地点和参与者:本基于人群的横断面研究使用了 1999 年至 2016 年全国健康和营养检查调查(NHANES)的数据。包括无乙型肝炎血清学检测结果缺失且有报告接种史的 2 至 18 岁美国出生者。数据分析于 2017 年 9 月至 2018 年 6 月进行。
报告完全接种乙型肝炎疫苗且具有阳性血清学检测结果表明具有免疫力的参与者比例。
在 21873 名儿童和青少年中,51.2%为男性,平均(SD)年龄为 10.6(4.6)岁。调查显示,乙型肝炎疫苗接种覆盖率从 1999 年到 2016 年显著增加(从 62.6%(95%CI,58.6%-66.4%)到 86.3%(95%CI,82.9%-89.2%);P<0.001)。在 2 至 5 岁儿童中,疫苗相关免疫也从 1999 年到 2016 年增加(从 60.7%(95%CI,48.8%-71.4%)到 65.2%(95%CI,57.4%-72.3%);P=0.001),但在 6 至 10 岁儿童中减少(从 64.6%(95%CI,57.7%-70.9%)到 46.5%(95%CI,39.1%-54.0%);P<0.001),11 至 13 岁青少年(从 68.8%(95%CI,58.1%-77.8%)到 26.2%(95%CI,18.6%-35.5%);P<0.001),以及 14 至 18 岁青少年(从 68.5%(95%CI,62.9%-73.6%)到 15.6%(95%CI,12.2%-19.8%);P<0.001)。按出生年份,1994-2003 年 NHANES 出生队列的疫苗相关免疫血清学证据显著下降,但在 1988 年至 1993 年之间出生的人群中则没有下降。非美国出生的儿童和青少年并没有表现出同样的免疫下降趋势。
在这项横断面研究中,尽管乙型肝炎疫苗接种率不断上升,但在 1994-2003 年 NHANES 出生队列中,美国出生的儿童和青少年的乙型肝炎免疫能力下降。这些发现表明,随着那些没有血清学免疫证据的人成为年轻人,他们可能会从事与感染风险增加相关的行为,因此可能需要对乙型肝炎进行监测和加强疫苗接种。