Hamami Dalila, Cameron Ross, Pollock Kevin G, Shankland Carron
Department of Computing Science, University of Oran1 Ahmed BenBellaOran, Algeria.
Health Protection ScotlandGlasgow, UK.
Front Physiol. 2017 Apr 25;8:233. doi: 10.3389/fphys.2017.00233. eCollection 2017.
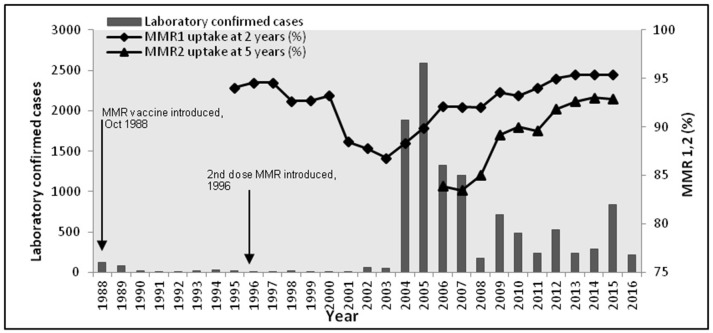
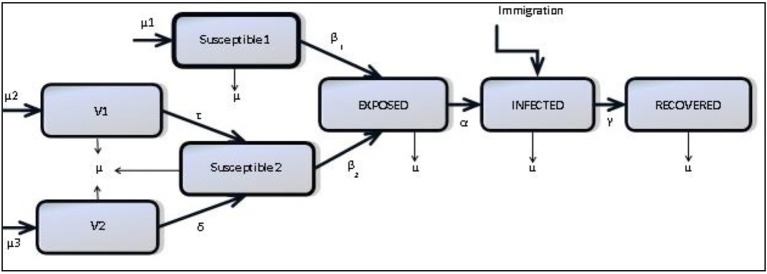
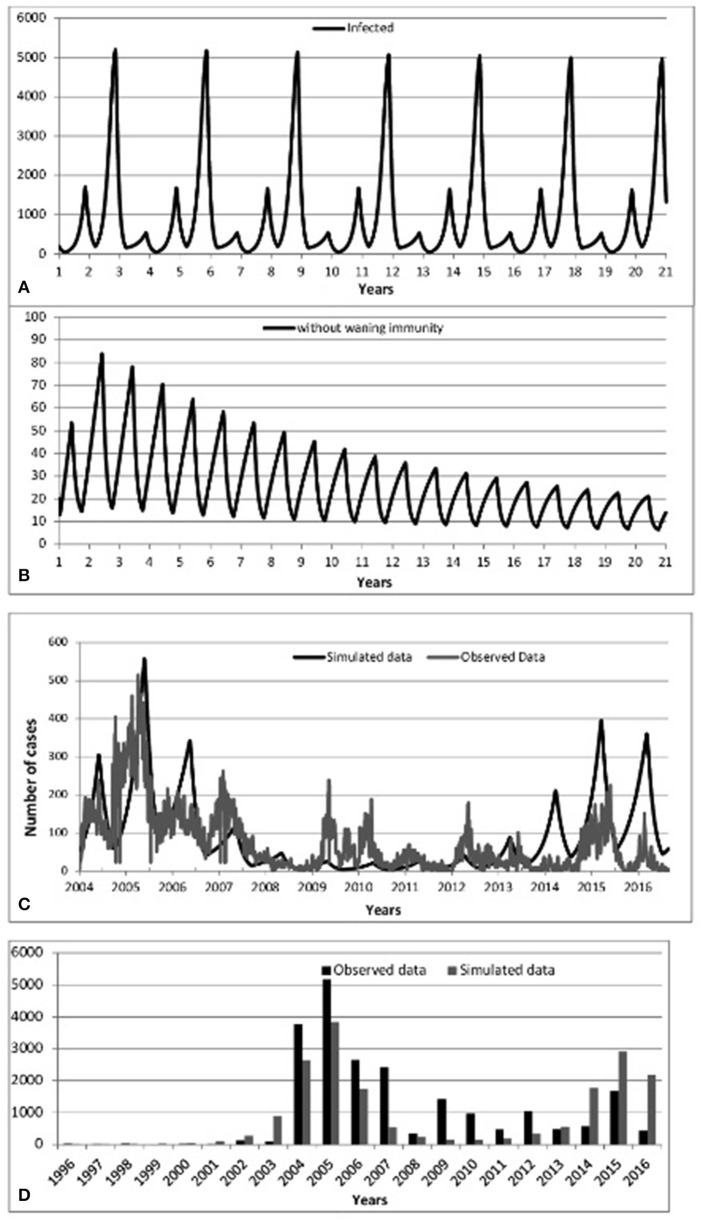
Vaccination programs for childhood diseases, such as measles, mumps and rubella have greatly contributed to decreasing the incidence and impact of those diseases. Nonetheless, despite long vaccination programmes across the world, mumps has not yet been eradicated in those countries: indeed, large outbreaks continue. For example, in Scotland large outbreaks occurred in 2004, 2005, and 2015, despite introducing the MMR (Measles-Mumps-Rubella) vaccine more than 20 years ago. There are indications that this vaccine-preventable disease is re-emerging in highly vaccinated populations. Here we investigate whether the resurgence of mumps is due to waning immunity, and further, could a booster dose be the solution to eradicate mumps or would it just extend the period of waning immunity? Using mathematical modeling we enhance a seasonally-structured disease model with four scenarios: no vaccination, vaccinated individuals protected for life, vaccinated individuals at risk of waning immunity, and introduction of measures to increase immunity (a third dose, or a better vaccine). The model is parameterised from observed clinical data in Scotland 2004-2015 and the literature. The results of the four scenarios are compared with observed clinical data 2004-2016. While the force of infection is relatively sensitive to the duration of immunity and the number of boosters undertaken, we conclude that periodic large outbreaks of mumps will be sustained for all except the second scenario. This suggests that the current protocol of two vaccinations is optimal in the sense that while there are periodic large outbreaks, the severity of cases in vaccinated individuals is less than in unvaccinated individuals, and the size of the outbreaks does not decrease sufficiently with a third booster to make economic sense. This recommendation relies on continuous efforts to maintain high levels of vaccination uptake.
针对麻疹、腮腺炎和风疹等儿童疾病的疫苗接种计划,对降低这些疾病的发病率和影响起到了巨大作用。尽管如此,尽管全球范围内开展了长期的疫苗接种计划,但在这些国家腮腺炎仍未被根除:事实上,大规模疫情仍在持续。例如,在苏格兰,尽管20多年前就引入了MMR(麻疹-腮腺炎-风疹)疫苗,但在2004年、2005年和2015年仍发生了大规模疫情。有迹象表明,这种疫苗可预防的疾病正在高疫苗接种率人群中再次出现。在此,我们研究腮腺炎的复发是否是由于免疫力下降所致,此外,一剂加强针能否成为根除腮腺炎的解决方案,还是只会延长免疫力下降的时期?我们使用数学建模,通过四种情景增强了一个季节性结构的疾病模型:不接种疫苗、接种疫苗的个体终身受到保护、接种疫苗的个体有免疫力下降的风险,以及引入增强免疫力的措施(第三剂或更好的疫苗)。该模型根据2004 - 2015年苏格兰的观察临床数据和文献进行参数化。将这四种情景的结果与2004 - 2016年的观察临床数据进行比较。虽然感染强度对免疫持续时间和接种的加强针数量相对敏感,但我们得出结论,除了第二种情景外,腮腺炎的周期性大规模疫情将持续存在。这表明,目前的两剂疫苗接种方案是最优的,因为虽然会有周期性的大规模疫情,但接种疫苗个体中的病例严重程度低于未接种疫苗的个体,而且第三剂加强针并不能使疫情规模充分减小到具有经济意义。这一建议依赖于持续努力维持高疫苗接种率。