Global Health Division, Menzies School of Health Research and Charles Darwin University, Darwin, Australia.
Centre for Child Health and Department of Child Health, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia.
PLoS Negl Trop Dis. 2020 Nov 11;14(11):e0008838. doi: 10.1371/journal.pntd.0008838. eCollection 2020 Nov.
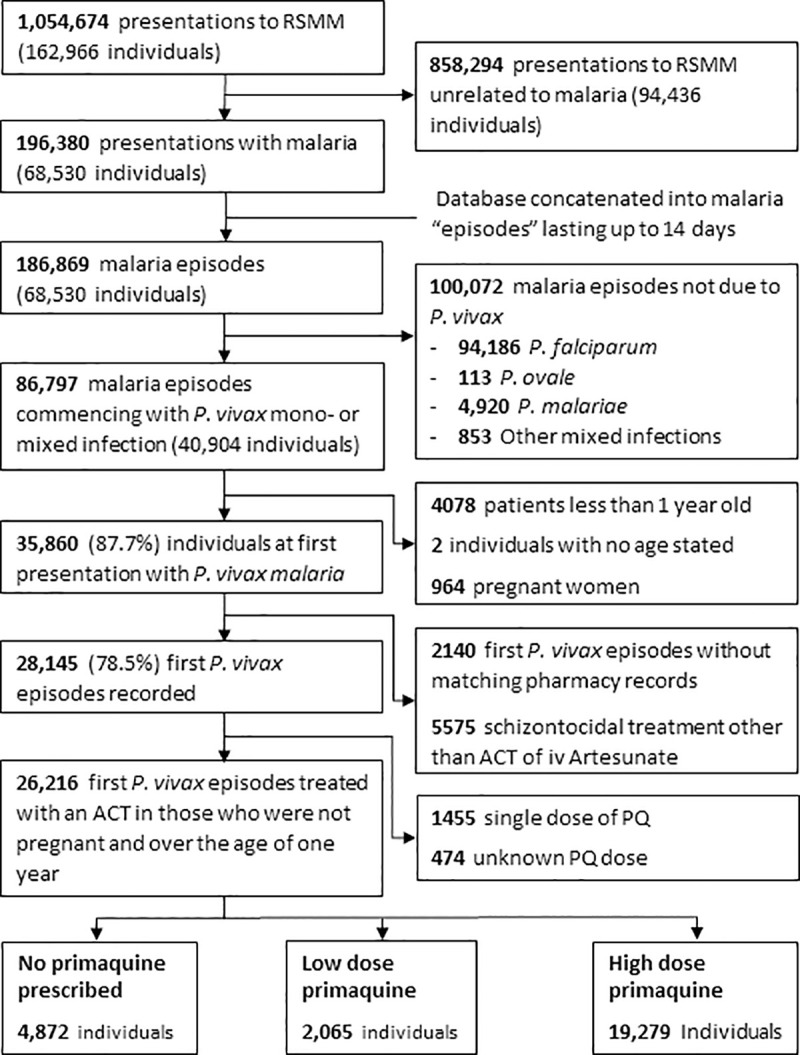
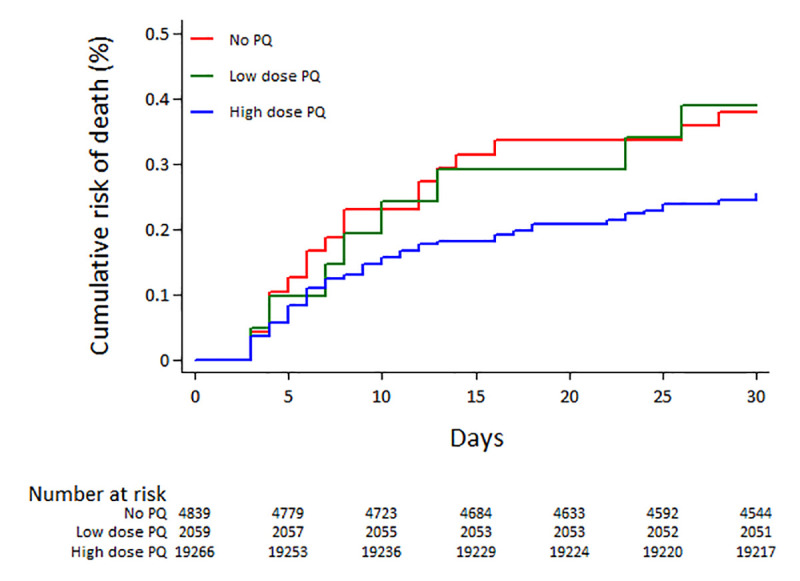
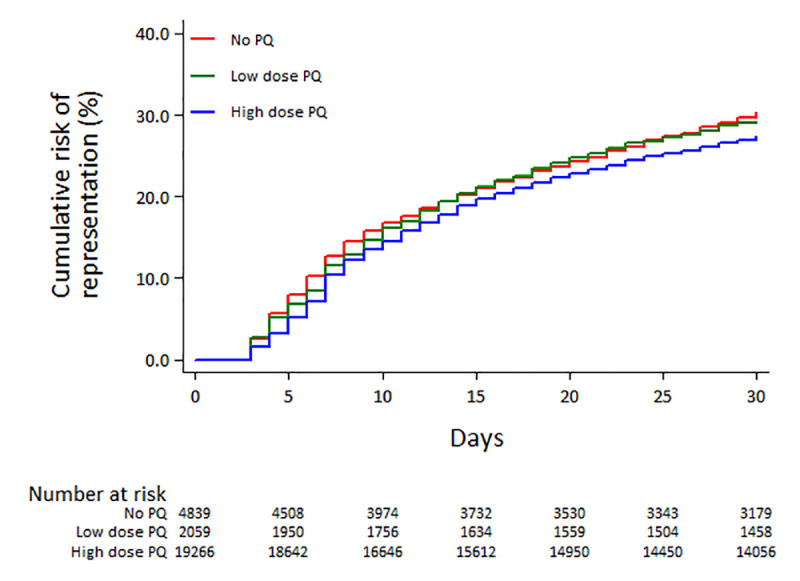
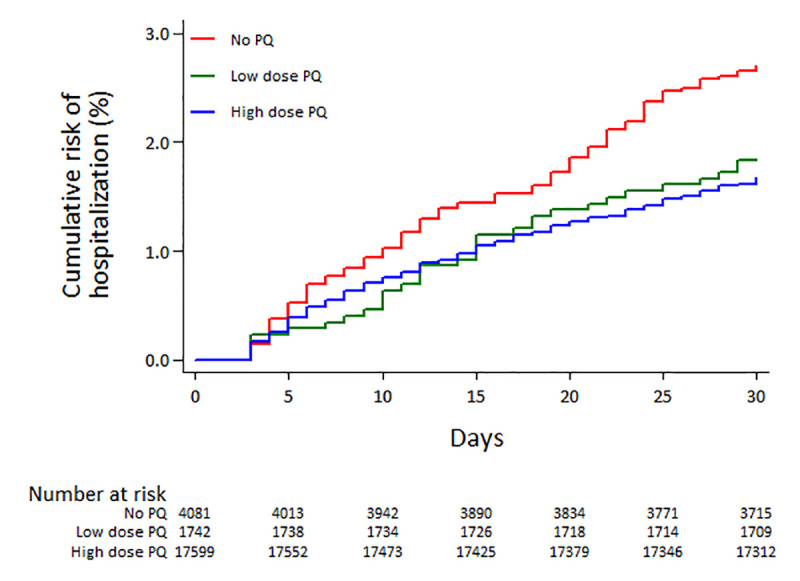
The widespread use of primaquine (PQ) radical cure for P. vivax, is constrained by concerns over its safety. We used routinely collected patient data to compare the overall morbidity and mortality in patients treated with and without PQ without prior testing of Glucose-6-Phosphate-Dehydrogenase (G6PD) deficiency in Papua, Indonesia, where there is a low prevalence of G6PD deficiency. Records were collated from patients older than 1 year, with P. vivax infection, who were treated with an artemisinin combination therapy (ACT). The risks of re-presentation, hospitalization, major fall in haemoglobin and death within 30 days were quantified and compared between patients treated with and without PQ using a Cox regression model. In total 26,216 patients with P. vivax malaria presented to the hospital with malaria during the study period. Overall 27.56% (95% Confidence Interval (95%CI): 26.96-28.16) of 21,344 patients treated with PQ re-presented with any illness within 30 days and 1.69% (1.51-1.88) required admission to hospital. The corresponding risks were higher in the 4,872 patients not treated with PQ; Adjusted Hazard Ratio (AHR) = 0.84 (0.79-0.91; p<0.001) and 0.54 (0.41-0.70; p<0.001) respectively. By day 30, 14.15% (12.45-16.05) of patients who had received PQ had a fall in haemoglobin (Hb) below 7g/dl compared to 20.43% (16.67-24.89) of patients treated without PQ; AHR = 0.66 (0.45-0.97; p = 0.033). A total of 75 (0.3%) patients died within 30 days of treatment with a mortality risk of 0.27% (0.21-0.35) in patients treated with PQ, compared to 0.38% (0.24-0.60) without PQ; AHR = 0.79 (0.43-1.45; p = 0.448). In Papua, Indonesia routine administration of PQ radical cure without prior G6PD testing, was associated with lower risk of all cause hospitalization and other serious adverse clinical outcomes. In areas where G6PD testing is not available or cannot be delivered reliably, the risks of drug induced haemolysis should be balanced against the potential benefits of reducing recurrent P. vivax malaria and its associated morbidity and mortality.
在印度尼西亚巴布亚,普遍使用伯氨喹(PQ)根治性治疗间日疟原虫,受到对其安全性的担忧的限制。我们使用常规收集的患者数据,比较了在没有预先检测葡萄糖-6-磷酸脱氢酶(G6PD)缺乏症的情况下,接受和未接受伯氨喹治疗的患者的总发病率和死亡率,那里的 G6PD 缺乏症患病率较低。记录来自 1 岁以上患有间日疟原虫感染的患者,他们接受了青蒿素联合疗法(ACT)治疗。使用 Cox 回归模型定量比较了接受和未接受 PQ 治疗的患者在 30 天内再次就诊、住院、血红蛋白大量下降和死亡的风险。在研究期间,共有 26216 名患有间日疟原虫疟疾的患者因疟疾到医院就诊。总体而言,21344 名接受 PQ 治疗的患者中有 27.56%(95%置信区间(95%CI):26.96-28.16)在 30 天内因任何疾病再次就诊,1.69%(1.51-1.88)需要住院治疗。在未接受 PQ 治疗的 4872 名患者中,相应的风险更高;调整后的危险比(AHR)为 0.84(0.79-0.91;p<0.001)和 0.54(0.41-0.70;p<0.001)。到第 30 天,接受 PQ 治疗的患者中有 14.15%(12.45-16.05)的血红蛋白(Hb)下降到 7g/dl 以下,而未接受 PQ 治疗的患者中有 20.43%(16.67-24.89);AHR = 0.66(0.45-0.97;p = 0.033)。共有 75 名(0.3%)患者在治疗后 30 天内死亡,接受 PQ 治疗的患者死亡率为 0.27%(0.21-0.35),而未接受 PQ 治疗的患者死亡率为 0.38%(0.24-0.60);AHR = 0.79(0.43-1.45;p = 0.448)。在印度尼西亚巴布亚,常规给予伯氨喹根治性治疗,而不进行 G6PD 检测,与全因住院和其他严重不良临床结局的风险降低相关。在无法进行或无法可靠提供 G6PD 检测的地区,药物诱导的溶血性贫血的风险应与减少复发性间日疟原虫疟疾及其相关发病率和死亡率的潜在益处相平衡。