Centre for Tropical Medicine and Global Health, Nuffield Department of Clinical Medicine, University of Oxford, Oxford, United Kingdom.
Mahidol-Oxford Tropical Medicine Research Unit, Mahidol University, Bangkok, Thailand.
Am J Trop Med Hyg. 2018 Feb;98(2):543-550. doi: 10.4269/ajtmh.17-0680. Epub 2017 Dec 21.
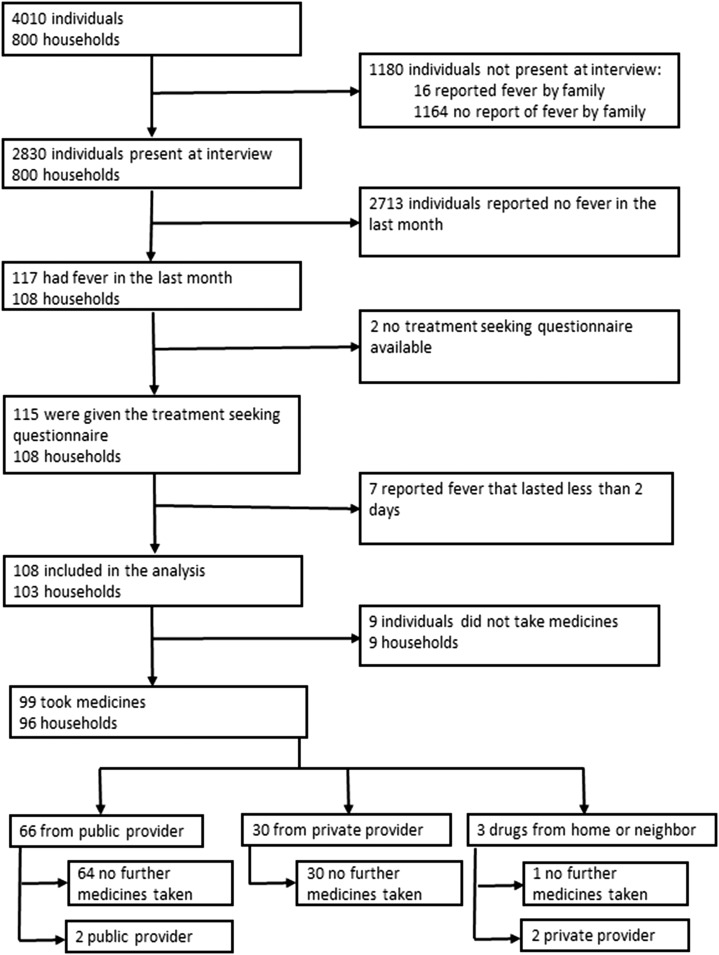
Artemisinin combination therapy is recommended for the treatment of multidrug resistant and . In March 2006, antimalarial policy in Indonesia was changed to a unified treatment with dihydroartemisinin-piperaquine for all species of malaria because of the low efficacy of previous drug treatments. In 2013, a randomized cross-sectional household survey in Papua was used to collect data on demographics, parasite positivity, treatment-seeking behavior, diagnosis and treatment of malaria, and household costs. Results were compared with a similar survey undertaken in 2005. A total of 800 households with 4,010 individuals were included in the 2013 survey. The prevalence of malaria parasitemia was 12% (348/2,795). Of the individuals who sought treatment of fever, 67% (66/98) reported attending a public provider at least once compared with 46% (349/764) before policy change ( < 0.001). During the 100 visits to healthcare providers, 95% (95) included a blood test for malaria and 74% (64/86) resulted in the recommended antimalarial for the diagnosed species, the corresponding figures before policy change were 48% (433/894) and 23% (78/336). The proportion of individuals seeking treatment more than once fell from 14% (107/764) before policy change to 2% (2/98) after policy change ( = 0.005). The mean indirect cost per fever episode requiring treatment seeking decreased from US$44.2 in 2005 to US$33.8 in 2013 ( = 0.006). The implementation of a highly effective antimalarial treatment was associated with better adherence of healthcare providers in both the public and private sectors and a reduction in clinical malaria and household costs.
青蒿素联合疗法被推荐用于治疗耐多药疟原虫和。2006 年 3 月,由于先前药物治疗效果不佳,印度尼西亚的抗疟政策改为对所有疟原虫物种采用统一的双氢青蒿素-哌喹治疗。2013 年,在巴布亚进行了一项随机横断面家庭调查,以收集人口统计学、寄生虫阳性率、寻求治疗行为、疟疾诊断和治疗以及家庭费用的数据。结果与 2005 年进行的类似调查进行了比较。2013 年的调查共包括 800 户家庭的 4010 人。疟原虫感染率为 12%(348/2795)。在因发热寻求治疗的人中,67%(66/98)报告至少一次去公共提供者就诊,而政策改变前为 46%(349/764)(<0.001)。在 100 次就诊中,95%(95/100)包括疟疾血液检查,74%(64/86)根据诊断出的物种开具推荐的抗疟药,政策改变前的相应数字为 48%(433/894)和 23%(78/336)。政策改变前寻求治疗超过一次的人数比例从 14%(107/764)降至政策改变后 2%(2/98)(=0.005)。每例发热需治疗的间接费用从 2005 年的 44.2 美元降至 2013 年的 33.8 美元(=0.006)。实施高效抗疟治疗与公共和私营部门的医疗服务提供者更好地遵守规定以及减少临床疟疾和家庭费用有关。