Department of General Practice and Emergency Medicine, Kathmandu University School of Medical Sciences, Dhulikhel, Nepal.
Department of Community Medicine, Kathmandu University School of Medical Sciences, Dhulikhel, Nepal.
BMC Psychiatry. 2020 Nov 11;20(1):533. doi: 10.1186/s12888-020-02910-8.
Depression is prevalent but poorly recognized in the Emergency Department (ED). We aimed to identify the frequency of unrecognized geriatric depression and its possible determinants in the ED using the 15-item geriatric depression scale (GDS). We also aimed to explore the performance of the shorter, five-item GDS as compared to the 15-item GDS.
This was a cross-sectional study of the ED patients ≥ 60 years. The previously validated Nepali version of GDS-15 screened the sample into "no", "mild-moderate" and "severe" depression using cutoff values of 4/5, and 8/9 respectively. Demographic and socioeconomic factors, comorbidities and health seeking behaviors were studied and the relation was assessed with binary (Chi-square and Kruskal-Wallis test) and multinomial regression analysis. The performance of GDS-5 was compared with the GDS-15 as standard. Cronbach's alpha was calculated to investigate reliability. Validity was assessed by calculating sensitivity, specificity, positive predictive value, negative predictive value, Spearman's correlation, receiver operating characteristic curve, and kappa coefficient.
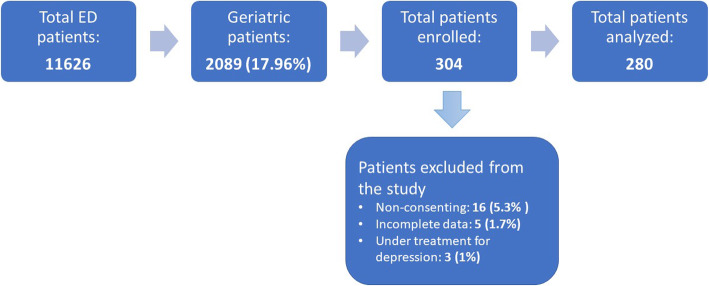
Two hundred eighty patients were enrolled with an overall prevalence of unrecognized depression of 45.7% [104 (81.3%) mild-moderate depression, and 24 (18.8%) severe depression]. The mean age of the sample was 71.36 with female predominance (61%), and 82.5% were illiterate. In the binary analysis, those who had more pain, visited the ED more often, had musculoskeletal diseases and sleep problems, mobility problems, visited local healers previously, and who reported self-perceived "heart and mind" disease showed statistically significant differences among the three categories. In multinomial regression analysis, visits to local healers, sleep problems and frequency of pain were significantly related to depression. The sensitivity, specificity, area under curve and Spearman's correlation of GDS-5 were 75.8%, 96%, 0.919, and 0.827 respectively. Cronbach's alpha for GDS-5 was low (0.416), therefore a new version was proposed which improved the sensitivity to 90.6% and Cronbach's alpha to 0.623.
Unrecognized geriatric depression was highly prevalent which urges the need for ED-based interventions for screening and referral. The proposed brief GDS-5 correlated well with the GDS-15 with better validity and internal reliability and offers a more expeditious form of screening for geriatric depression in emergency settings in Nepal.
抑郁在急诊科(ED)很普遍,但识别率低。我们旨在使用 15 项老年抑郁量表(GDS)来确定 ED 中未被识别的老年抑郁症的频率及其可能的决定因素。我们还旨在探索更短的五分量表 GDS 与 15 分量表 GDS 的表现。
这是一项对年龄≥60 岁的 ED 患者的横断面研究。经过验证的尼泊尔语版本的 GDS-15 使用 4/5 和 8/9 的截值将样本分为“无”、“轻度-中度”和“重度”抑郁。研究了人口统计学和社会经济因素、合并症和寻求健康行为,并使用二项式(卡方和克鲁斯卡尔-沃利斯检验)和多项回归分析评估了这些因素与抑郁的关系。GDS-5 的性能与标准的 GDS-15 进行了比较。计算克朗巴赫α值以评估可靠性。通过计算敏感性、特异性、阳性预测值、阴性预测值、斯皮尔曼相关系数、接收者操作特征曲线和kappa 系数来评估有效性。
共纳入 280 例患者,未识别的抑郁症总患病率为 45.7%[104 例(81.3%为轻度-中度抑郁,24 例(18.8%)为重度抑郁]。样本的平均年龄为 71.36 岁,女性居多(61%),82.5%为文盲。在二项分析中,那些疼痛更严重、去 ED 就诊更频繁、患有肌肉骨骼疾病和睡眠问题、有行动问题、以前曾去当地治疗师就诊以及报告自我感知的“心身”疾病的患者,在三个类别中显示出统计学上的显著差异。在多项回归分析中,去当地治疗师就诊、睡眠问题和疼痛频率与抑郁显著相关。GDS-5 的敏感性、特异性、曲线下面积和斯皮尔曼相关系数分别为 75.8%、96%、0.919 和 0.827。GDS-5 的克朗巴赫α值较低(0.416),因此提出了一个新的版本,将敏感性提高到 90.6%,克朗巴赫α值提高到 0.623。
未被识别的老年抑郁症患病率很高,这迫切需要在 ED 进行基于干预的筛查和转诊。建议的简短 GDS-5 与 GDS-15 相关性良好,具有更好的有效性和内部可靠性,并为尼泊尔急诊环境中的老年抑郁症提供了更快捷的筛查形式。