Department of Medicine, NUI Galway, Galway, Ireland.
Department of Medicine, Population Health Research Institute, McMaster University and Hamilton Health Sciences, Hamilton, Ontario, Canada.
Am J Hypertens. 2021 Apr 20;34(4):414-425. doi: 10.1093/ajh/hpaa176.
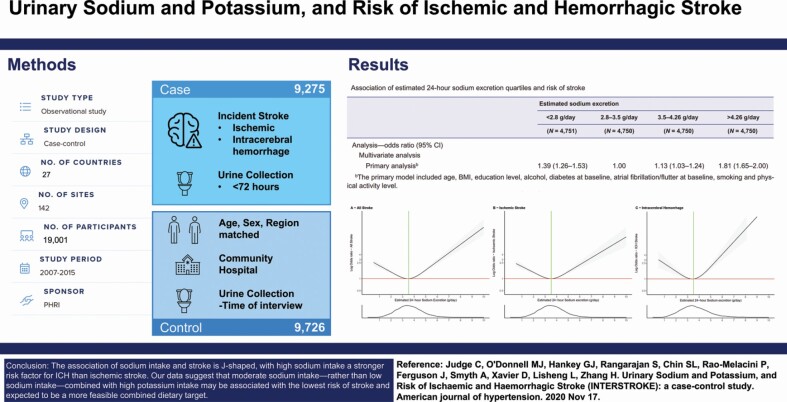
Although low sodium intake (<2 g/day) and high potassium intake (>3.5 g/day) are proposed as public health interventions to reduce stroke risk, there is uncertainty about the benefit and feasibility of this combined recommendation on prevention of stroke.
We obtained random urine samples from 9,275 cases of acute first stroke and 9,726 matched controls from 27 countries and estimated the 24-hour sodium and potassium excretion, a surrogate for intake, using the Tanaka formula. Using multivariable conditional logistic regression, we determined the associations of estimated 24-hour urinary sodium and potassium excretion with stroke and its subtypes.
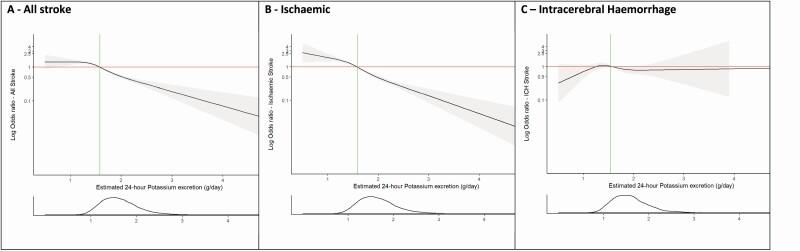
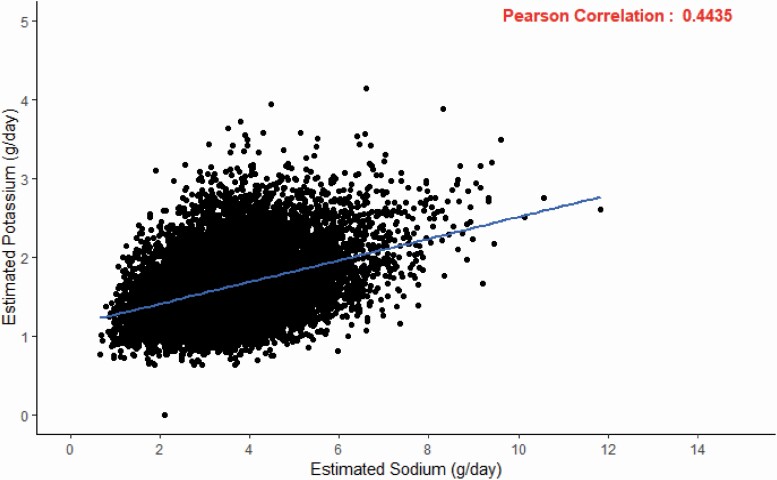
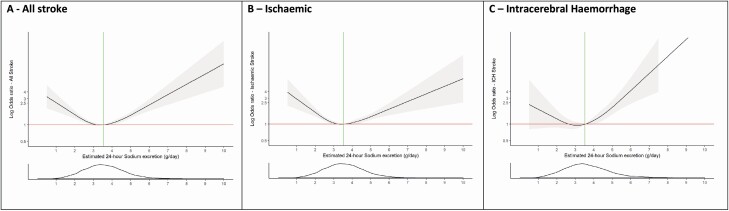
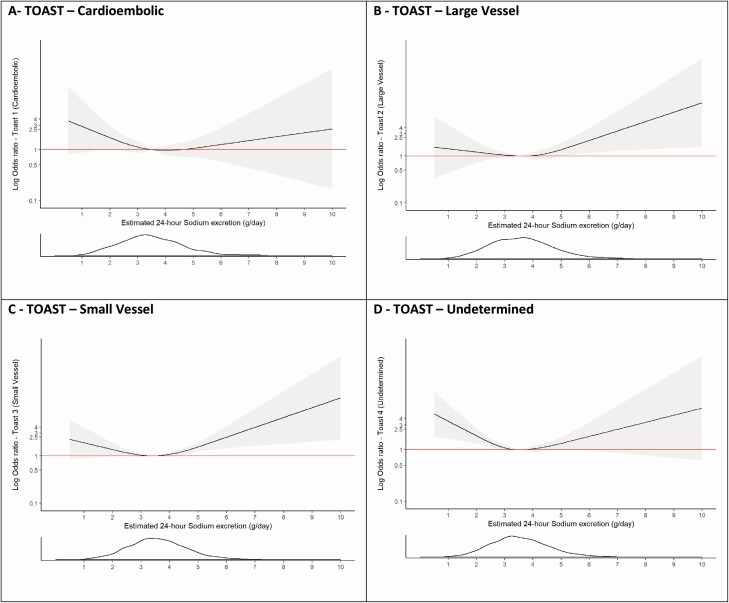
Compared with an estimated urinary sodium excretion of 2.8-3.5 g/day (reference), higher (>4.26 g/day) (odds ratio [OR] 1.81; 95% confidence interval [CI], 1.65-2.00) and lower (<2.8 g/day) sodium excretion (OR 1.39; 95% CI, 1.26-1.53) were significantly associated with increased risk of stroke. The stroke risk associated with the highest quartile of sodium intake (sodium excretion >4.26 g/day) was significantly greater (P < 0.001) for intracerebral hemorrhage (ICH) (OR 2.38; 95% CI, 1.93-2.92) than for ischemic stroke (OR 1.67; 95% CI, 1.50-1.87). Urinary potassium was inversely and linearly associated with risk of stroke, and stronger for ischemic stroke than ICH (P = 0.026). In an analysis of combined sodium and potassium excretion, the combination of high potassium intake (>1.58 g/day) and moderate sodium intake (2.8-3.5 g/day) was associated with the lowest risk of stroke.
The association of sodium intake and stroke is J-shaped, with high sodium intake a stronger risk factor for ICH than ischemic stroke. Our data suggest that moderate sodium intake-rather than low sodium intake-combined with high potassium intake may be associated with the lowest risk of stroke and expected to be a more feasible combined dietary target.
尽管低钠摄入(<2 克/天)和高钾摄入(>3.5 克/天)被提议作为减少中风风险的公共卫生干预措施,但对于这种联合建议在预防中风方面的益处和可行性仍存在不确定性。
我们从 27 个国家的 9275 例急性首发中风病例和 9726 例匹配对照中获得了随机尿样,并使用 Tanaka 公式估算了 24 小时钠和钾的排泄量,这是摄入量的替代指标。使用多变量条件逻辑回归,我们确定了估计的 24 小时尿钠和钾排泄与中风及其亚型之间的关联。
与估计的 2.8-3.5 克/天(参考值)的尿钠排泄相比,更高(>4.26 克/天)(比值比[OR]1.81;95%置信区间[CI]1.65-2.00)和更低(<2.8 克/天)的尿钠排泄(OR 1.39;95%CI,1.26-1.53)与中风风险增加显著相关。与最高四分位钠摄入量(尿钠排泄>4.26 克/天)相关的中风风险,对于脑出血(ICH)(OR 2.38;95%CI,1.93-2.92)明显大于(P<0.001)对于缺血性中风(OR 1.67;95%CI,1.50-1.87)。尿钾与中风风险呈负相关,且与缺血性中风相比,与 ICH 的相关性更强(P=0.026)。在钠和钾排泄联合分析中,高钾摄入(>1.58 克/天)和中等钠摄入(2.8-3.5 克/天)的组合与中风风险最低相关。
钠摄入量与中风的关系呈 J 型,高钠摄入是 ICH 的风险因素,比缺血性中风更强。我们的数据表明,中等钠摄入而不是低钠摄入与高钾摄入相结合可能与中风风险最低相关,并且预计这将是一个更可行的联合饮食目标。