Northwestern University, Chicago, Illinois; Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, Illinois.
Northwestern University, Chicago, Illinois.
J Am Soc Echocardiogr. 2021 Apr;34(4):388-400. doi: 10.1016/j.echo.2020.11.002. Epub 2020 Nov 17.
Little is known about the timing of preclinical heart failure (HF) development, particularly among blacks. The primary aims of this study were to delineate age-related left ventricular (LV) structure and function evolution in a biracial cohort and to test the hypothesis that young-adult LV parameters within normative ranges would be associated with incident stage B-defining LV abnormalities over 25 years, independent of cumulative risk factor burden.
Data from the Coronary Artery Risk Development in Young Adults study were analyzed. Participants (n = 2,833) had a mean baseline age of 30.1 years; 45% were black, and 56% were women. Generalized estimating equation logistic regression was used to estimate age-related probabilities of stage B LV abnormalities (remodeling, hypertrophy, or dysfunction) and logistic regression to examine risk factor-adjusted associations between baseline LV parameters and incident abnormalities. Cox regression was used to assess whether baseline LV parameters associated with incident stage B LV abnormalities were also associated with incident clinical (stage C/D) HF events over >25 years' follow-up.
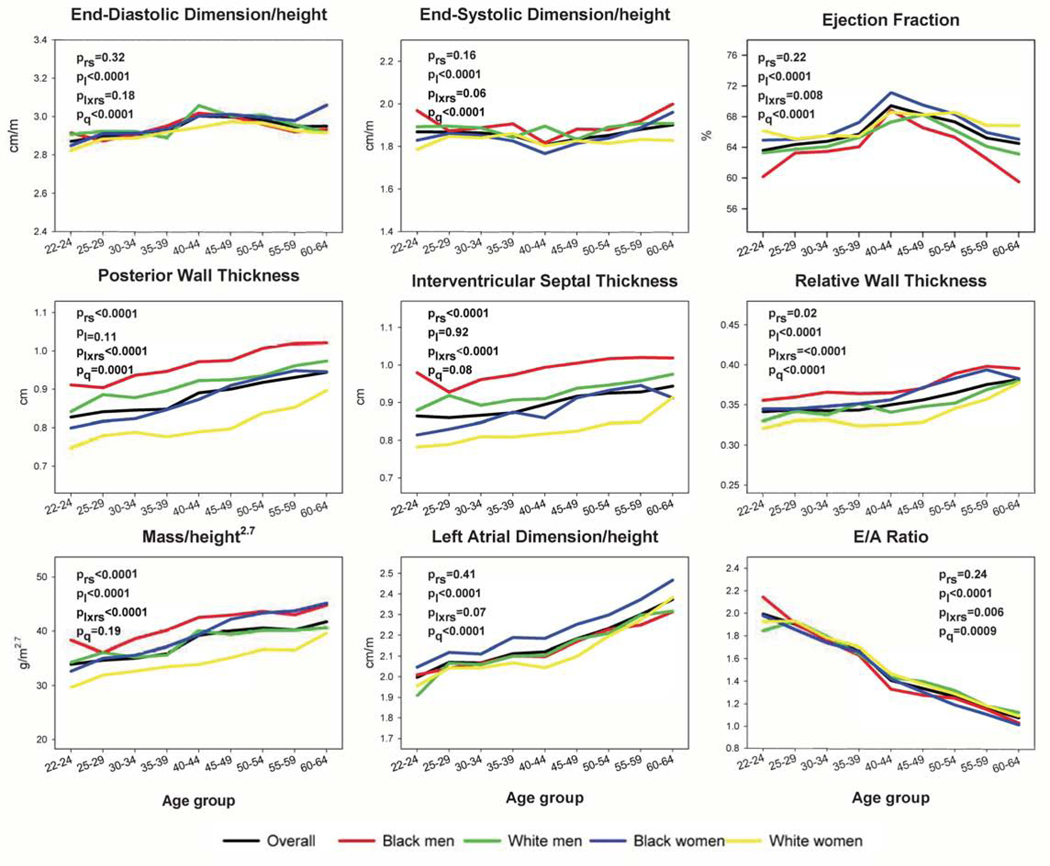
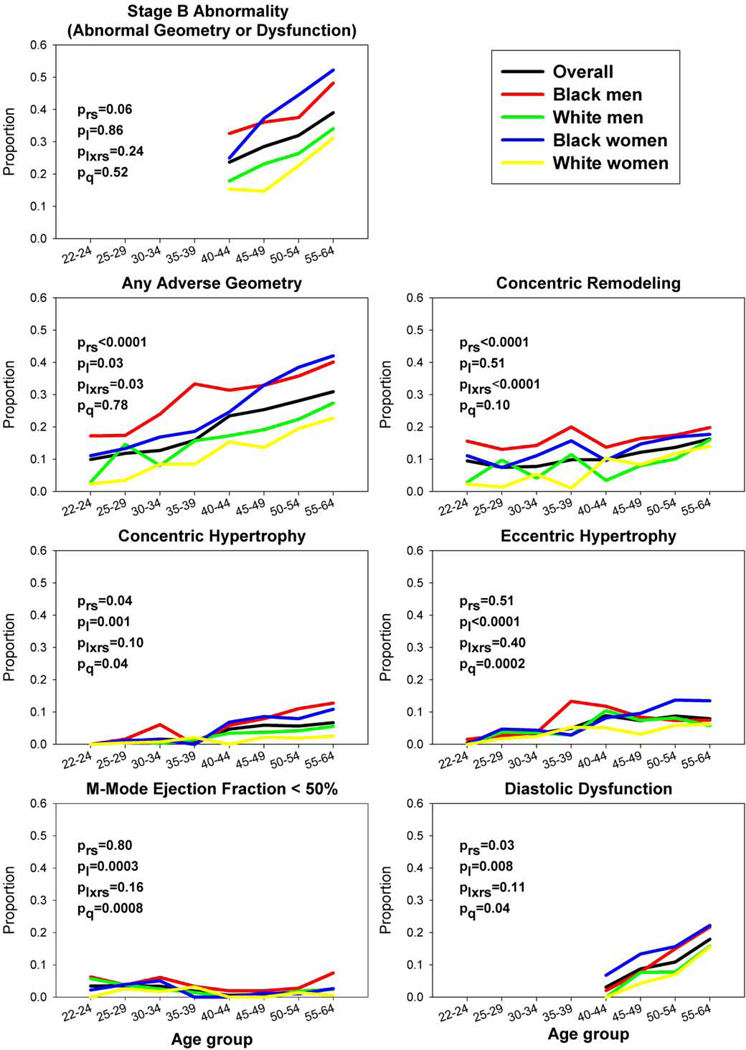
Probabilities of stage B LV abnormalities at ages 25 and 60 years were 10.5% (95% CI, 9.4%-11.8%) and 45.0% (95% CI, 42.0%-48.1%), with significant race-sex disparities (e.g., at age 60, black men 52.7% [95% CI, 44.9%-60.3%], black women 59.4% [95% CI, 53.6%-65.0%], white men 39.1% [95% CI, 33.4%-45.0%], and white women 39.1% [95% CI, 33.9%-44.6%]). Over 25 years, baseline LV end-systolic dimension indexed to height was associated with incident systolic dysfunction (adjusted odds ratio per 1 SD higher, 2.56; 95% CI, 1.87-3.52), eccentric hypertrophy (1.34; 95% CI, 1.02-1.75), concentric hypertrophy (0.69; 95% CI, 0.51-0.91), and concentric remodeling (0.68; 95% CI, 0.58-0.79); baseline LV mass indexed to height was associated with incident eccentric hypertrophy (1.70; 95% CI, 1.25-2.32]), concentric hypertrophy (1.63; 95% CI, 1.19-2.24), and diastolic dysfunction (1.24; 95% CI, 1.01-1.52). Among the entire cohort with baseline echocardiographic data available (n = 4,097; 72 HF events), LV end-systolic dimension indexed to height and LV mass indexed to height were significantly associated with incident clinical HF (adjusted hazard ratios per 1 SD higher, 1.56 [95% CI, 1.26-1.93] and 1.42 [95% CI, 1.14-1.75], respectively).
Stage B LV abnormalities and related racial disparities were present in young adulthood, increased with age, and were associated with baseline variation in indexed LV end-systolic dimension and mass. Baseline indexed LV end-systolic dimension and mass were also associated with incident clinical HF. Efforts to prevent the LV abnormalities underlying clinical HF should start from a young age.
对于心力衰竭(HF)的发生,尤其是在黑人中,其在临床前阶段的发生时间知之甚少。本研究的主要目的是描述一个双种族队列中与年龄相关的左心室(LV)结构和功能演变,并检验以下假设,即在 25 年的随访中,年轻成年人的 LV 参数在正常范围内,与 25 年后发生 B 期定义的 LV 异常(重塑、肥大或功能障碍)相关,而与累积风险因素负担无关。
分析了来自冠状动脉风险发展在年轻人研究的数据。参与者(n=2833)的平均基线年龄为 30.1 岁;45%为黑人,56%为女性。使用广义估计方程逻辑回归估计 B 期 LV 异常(重塑、肥大或功能障碍)的年龄相关概率,并使用逻辑回归检查基线 LV 参数与新发异常之间的风险因素调整关联。Cox 回归用于评估基线 LV 参数与新发 B 期 LV 异常相关的个体是否也与 >25 年随访期间发生的临床(C/D 期)HF 事件相关。
在 25 岁和 60 岁时,B 期 LV 异常的概率分别为 10.5%(95%CI,9.4%-11.8%)和 45.0%(95%CI,42.0%-48.1%),且存在显著的种族-性别差异(例如,在 60 岁时,黑人男性 52.7%[95%CI,44.9%-60.3%],黑人女性 59.4%[95%CI,53.6%-65.0%],白人男性 39.1%[95%CI,33.4%-45.0%],和白人女性 39.1%[95%CI,33.9%-44.6%])。在 25 年的随访中,基线 LV 收缩末期内径与身高的比值与新发收缩功能障碍相关(每 1 SD 更高的调整优势比,2.56;95%CI,1.87-3.52)、偏心肥大(1.34;95%CI,1.02-1.75)、向心性肥大(0.69;95%CI,0.51-0.91)和向心性重塑(0.68;95%CI,0.58-0.79);基线 LV 质量与身高的比值与新发偏心肥大(1.70;95%CI,1.25-2.32))、向心性肥大(1.63;95%CI,1.19-2.24)和舒张功能障碍(1.24;95%CI,1.01-1.52)相关。在有基线超声心动图数据的整个队列中(n=4097;72 例 HF 事件),LV 收缩末期内径与身高的比值和 LV 质量与身高的比值与临床 HF 的发生显著相关(每 1 SD 更高的调整危险比,1.56[95%CI,1.26-1.93]和 1.42[95%CI,1.14-1.75])。
B 期 LV 异常及其相关的种族差异在年轻时就存在,随年龄增长而增加,并与基线 LV 收缩末期内径和质量的指数变化相关。基线 LV 收缩末期内径和质量也与临床 HF 的发生相关。预防临床 HF 潜在的 LV 异常应从年轻时开始。