Department of Diabetes, Endocrinology, and Metabolism Center Hospital National Center for Global Health and Medicine Tokyo Japan.
Department of Diabetes and Endocrinology Toranomon Hospital Kajigaya Kanagawa Japan.
J Am Heart Assoc. 2020 Dec;9(23):e018827. doi: 10.1161/JAHA.120.018827. Epub 2020 Nov 23.
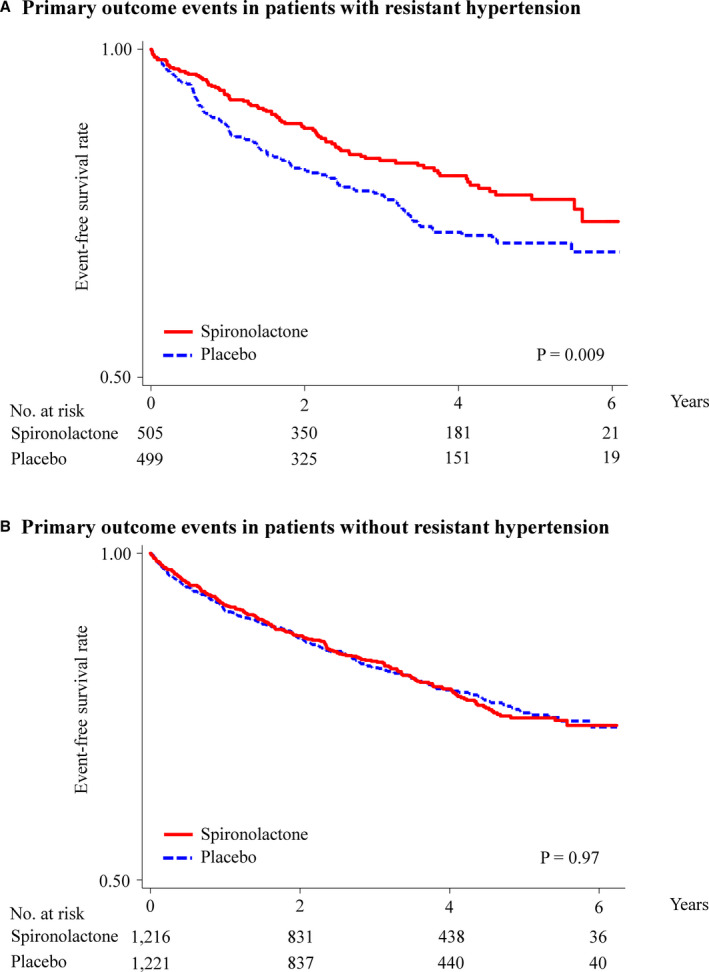
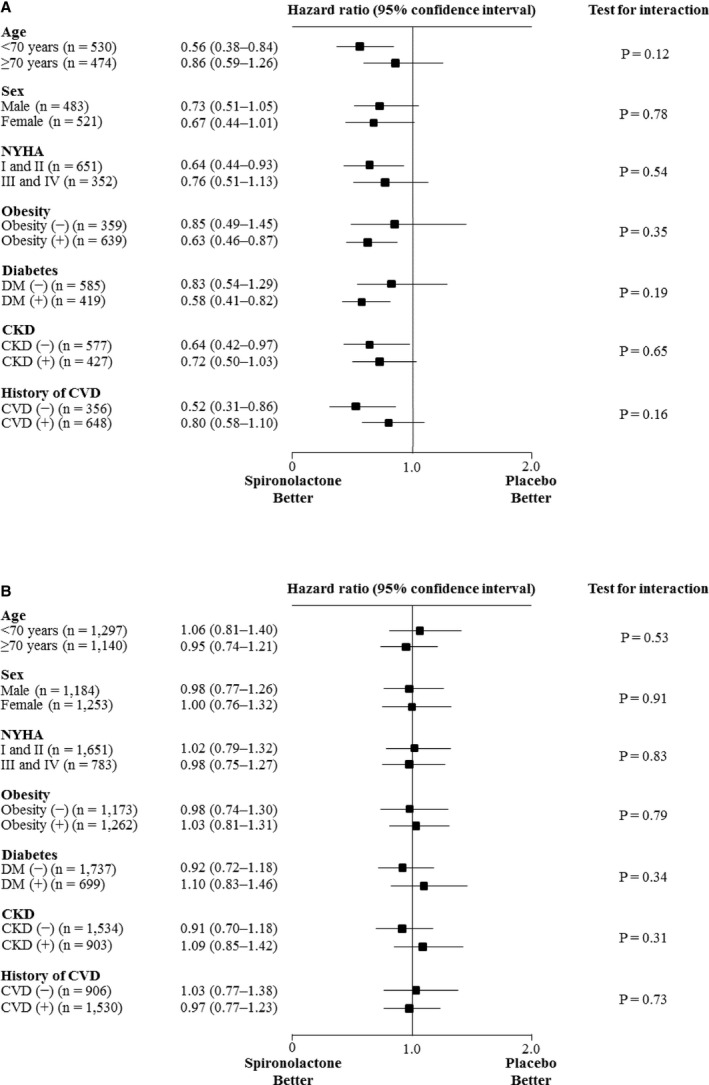
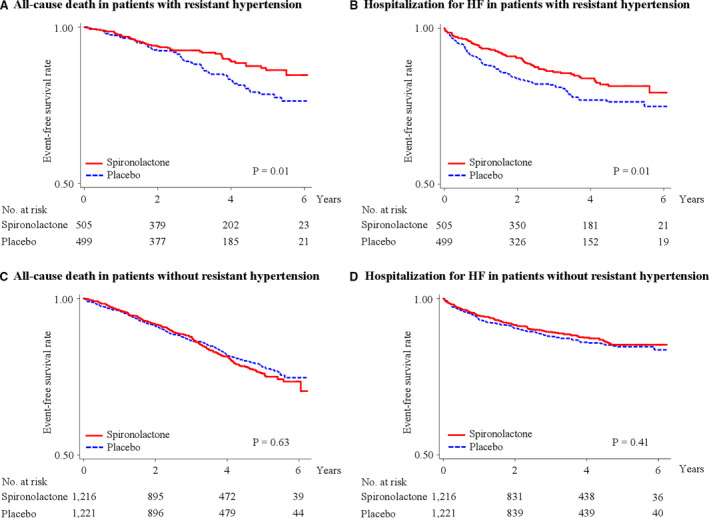
Background Resistant hypertension is a salt-retaining condition possibly attributable to inappropriate aldosterone secretion. Methods and Results This study was a secondary analysis of the TOPCAT (Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist) trial. Patients with heart failure with preserved ejection fraction (HFpEF) with (n=1004) and without (n=2437) resistant hypertension were included. Resistant hypertension was defined as systolic blood pressure ≥130 mm Hg and/or diastolic blood pressure ≥80 mm Hg in a patient with hypertension, despite the concurrent use of a renin-angiotensin system blocker (angiotensin-converting enzyme inhibitor/angiotensin receptor blocker), a calcium channel blocker, and a diuretic; or as those patients using ≥4 classes of antihypertensive medication. The primary outcome was a composite of cardiovascular death, aborted cardiac arrest, or heart failure hospitalization. We analyzed hazard ratios (HRs) for outcomes with 95% CIs in the spironolactone group and compared them with the placebo group using Cox proportional hazard models. The risk of primary outcome events in patients with HFpEF with resistant hypertension was significantly lower in the spironolactone group than in the placebo group (HR, 0.70; 95% CI, 0.53-0.91; =0.009), whereas the risk of primary outcome events in patients with HFpEF without resistant hypertension was not significantly different between the 2 groups (HR, 1.00; 95% CI, 0.83-1.20; =0.97). There was a significant interaction between spironolactone use and resistant hypertension (=0.03). Similar associations were also observed in patients with HFpEF from the Americas (United States, Canada, Brazil, and Argentina) only. Conclusions Spironolactone may be an effective add-on medication for patients with HFpEF with resistant hypertension taking angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, calcium channel blockers, and diuretics.
抵抗性高血压是一种保钠状态,可能归因于醛固酮分泌不当。
本研究是 TOPCAT(醛固酮拮抗剂治疗保留射血分数心力衰竭)试验的二次分析。纳入了射血分数保留的心力衰竭(HFpEF)伴(n=1004)和不伴(n=2437)抵抗性高血压的患者。抵抗性高血压定义为高血压患者的收缩压≥130mmHg 和/或舒张压≥80mmHg,尽管同时使用肾素-血管紧张素系统阻滞剂(血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂)、钙通道阻滞剂和利尿剂;或使用≥4 类降压药物的患者。主要结局是心血管死亡、心搏骤停未遂或心力衰竭住院的复合结局。我们使用 Cox 比例风险模型分析螺内酯组的结局风险比(HR)及其 95%置信区间,并与安慰剂组进行比较。HFpEF 伴抵抗性高血压患者螺内酯组的主要结局事件风险明显低于安慰剂组(HR,0.70;95%CI,0.53-0.91;=0.009),而 HFpEF 不伴抵抗性高血压患者两组之间的主要结局事件风险无显著差异(HR,1.00;95%CI,0.83-1.20;=0.97)。螺内酯的使用与抵抗性高血压之间存在显著的交互作用(=0.03)。仅在来自美洲(美国、加拿大、巴西和阿根廷)的 HFpEF 患者中也观察到了类似的关联。
螺内酯可能是一种有效的附加药物,适用于服用血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂、钙通道阻滞剂和利尿剂的 HFpEF 伴抵抗性高血压患者。