Ceresa Iride Francesca, Savioli Gabriele, Angeli Valentina, Novelli Viola, Muzzi Alba, Grugnetti Giuseppina, Cobianchi Lorenzo, Manzoni Federica, Klersy Catherine, Lago Paolo, Marchese Pierantonio, Marena Carlo, Ricevuti Giovanni, Bressan Maria Antonietta
Emergency Department, San Matteo IRCCS Hospital Foundation, Pavia 27100, Italy.
Department of Clinical-Surgical, Diagnostic and Pediatric Sciences, PhD School in Experimental Medicine, University of Pavia, Pavia 27100, Italy.
Open Access Emerg Med. 2020 Nov 16;12:377-387. doi: 10.2147/OAEM.S267069. eCollection 2020.
The sudden increase in the number of critically ill patients following a disaster can be overwhelming.
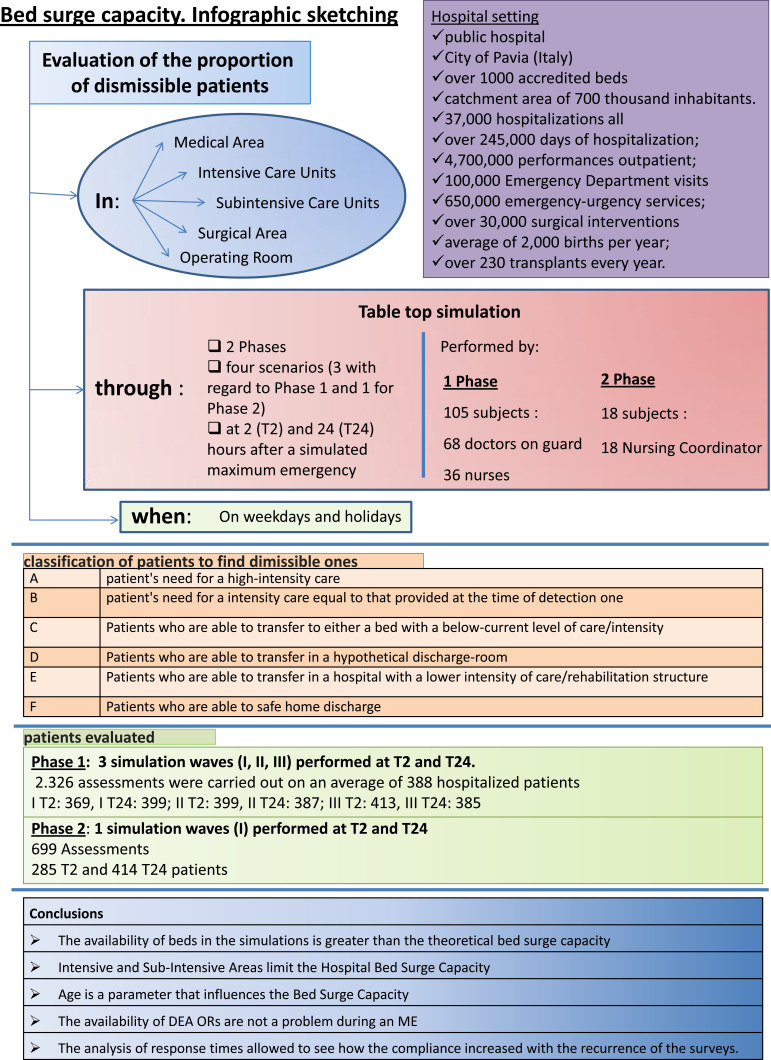
The main objective of this study was to assess the real number of available and readily freeable beds ("bed surge capacity") and the availability of emergency operating rooms (OR) in a maximum emergency using a theoretical simulation.
The proportion of dismissible patients in four areas (Medical Area, Surgical Area, Sub-intensive Care Units, Intensive Care Units) and three emergency OR was assessed at 2 and 24 hours after a simulated maximum emergency. Four scenarios were modeled. Hospitalization and surgical capacities were assessed on weekdays and holidays. The creation of new beds was presumed by the possibility of moving patients to a lower level of care than that provided at the time of detection, of dislocation of patients to a discharge room, with care transferred to lower-intensity hospitals, rehabilitation, or discharge facilities. The Phase 1 table-top simulations were conducted during the weekday morning hours. In particular, the 24-hour table-top simulations of a hypothetical event lasted about 150 minutes compared to those conducted at 2 hours, which were found to be longer (about 195 minutes). Phase 2 was conducted on two public holidays and a quick response time was observed within the first 40 minutes of the start of the test (about 45% of departments).
The availability of simulated beds was greater than that indicated in the maximum emergency plans (which was based solely on the census of beds). Patients admitted to Intensive Care and The Sub-Intensive Area may be more difficult to move than those in low-intensity care. The availability of emergency OR was not problematic. Age influenced the possibility of remitting/transferring patients.
Simulation in advance of a maximum emergency is helpful in designing an efficient response plan.
灾难后危重症患者数量的突然增加可能是压倒性的。
本研究的主要目的是通过理论模拟评估在最大紧急情况下可用且可立即腾出的床位的实际数量(“床位激增能力”)以及急诊手术室的可用性。
在模拟最大紧急情况后的2小时和24小时,评估四个区域(医疗区、手术区、亚重症监护病房、重症监护病房)和三个急诊手术室中可出院患者的比例。模拟了四种情景。在工作日和节假日评估住院和手术能力。通过将患者转移到比发现时提供的护理级别更低的护理级别、将患者转移到出院室、将护理转移到低强度医院、康复或出院设施的可能性来假定新床位的创建。第一阶段的桌面模拟在工作日上午进行。特别是,与2小时时进行的模拟相比,假设事件的24小时桌面模拟持续约150分钟,发现前者更长(约195分钟)。第二阶段在两个公共假日进行,在测试开始后的前40分钟内观察到快速响应时间(约45%的科室)。
模拟床位的可用性大于最大应急计划中指出的可用性(最大应急计划仅基于床位普查)。入住重症监护病房和亚重症监护区的患者可能比低强度护理患者更难转移。急诊手术室的可用性没有问题。年龄影响患者缓解/转移的可能性。
在最大紧急情况之前进行模拟有助于设计有效的应对计划。