Savioli Gabriele, Ceresa Iride Francesca, Luzzi Sabino, Giotta Lucifero Alice, Pioli Di Marco Maria Serena, Manzoni Federica, Preda Lorenzo, Ricevuti Giovanni, Bressan Maria Antonietta
Emergency Department, Fondazione IRCCS Policlinico San Matteo, 27100 Pavia, Italy.
PhD School in Experimental Medicine, Department of Clinical-Surgical, Diagnostic and Pediatric Sciences, University of Pavia, 27100 Pavia, Italy.
Medicina (Kaunas). 2021 Apr 7;57(4):357. doi: 10.3390/medicina57040357.
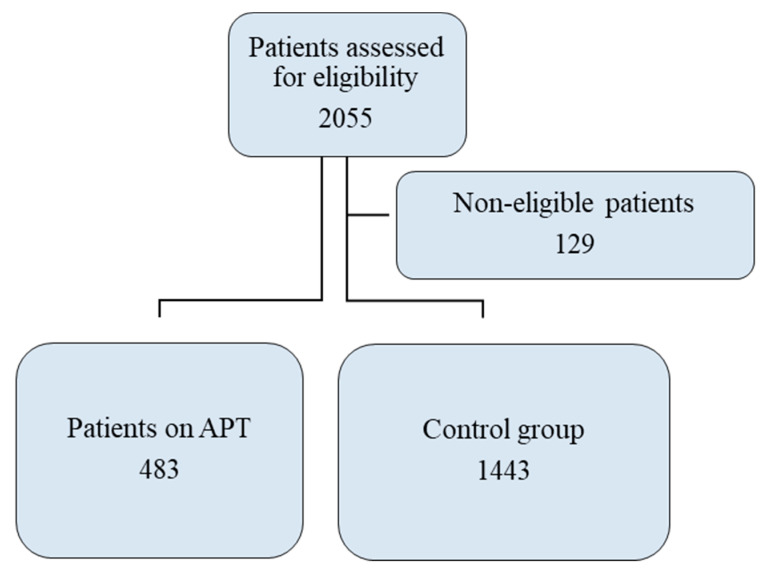
In patients who receive antiplatelet therapy (APT), the bleeding risk profile after mild head trauma (MHT) still needs clarification. Some studies have demonstrated an association with bleeding risk, whereas others have not. We studied the population of our level II emergency department (ED) trauma center to determine the risk of bleeding in patients receiving APT and whether bleeding results not from antiplatelet agents but rather from age. We assessed the bleeding risk, the incidence of intracranial hemorrhage (ICH) that necessitated hospitalization for observation, the need for cranial neurosurgery, the severity of the patient's condition at discharge, and the frequency of ED revisits for head trauma in patients receiving APT. This retrospective single-center study included 483 patients receiving APT who were in the ED for MHT in 2019. The control group consisted of 1443 patients in the ED with MHT over the same period who were not receiving APT or anticoagulant therapy. Our ED diagnostic therapeutic protocol mandates both triage and the medical examination to identify patients with MHT who are taking any anticoagulant or APT. APT was not significantly associated with bleeding risk ( > 0.05); as a risk factor, age was significantly associated with the risk of bleeding, even after adjustment for therapy. Patients receiving APT had a greater need of surgery (1.2% vs. 0.4%; < 0.0001) and a higher rate of hospitalization (52.9% vs. 37.4%; < 0.0001), and their clinical condition was more severe (evaluated according to the exit code value on a one-dimensional quantitative five-point numerical scale) at the time of discharge ( = 0.013). The frequency of ED revisits due to head trauma did not differ between the two groups. The risk of bleeding in patients receiving APT who had MHT was no higher than that in the control group. However, the clinical condition of patients receiving APT, including hospital admission for ICH monitoring and cranial neurosurgical interventions, was more severe.
在接受抗血小板治疗(APT)的患者中,轻度头部创伤(MHT)后的出血风险情况仍有待明确。一些研究已证实其与出血风险有关,而其他研究则未发现这种关联。我们对我院二级急诊科创伤中心的人群进行了研究,以确定接受APT治疗的患者的出血风险,以及出血是否并非由抗血小板药物引起,而是由年龄导致。我们评估了接受APT治疗的患者的出血风险、因颅内出血(ICH)而需要住院观察的发生率、进行颅脑神经外科手术的必要性、出院时患者的病情严重程度以及因头部创伤返回急诊科复诊的频率。这项回顾性单中心研究纳入了2019年因MHT在急诊科就诊的483例接受APT治疗的患者。对照组由同期在急诊科因MHT就诊但未接受APT或抗凝治疗的1443例患者组成。我们急诊科的诊断治疗方案要求进行分诊和体格检查,以识别正在服用任何抗凝剂或APT的MHT患者。APT与出血风险无显著关联(>0.05);作为一个风险因素,即使在对治疗进行调整后,年龄仍与出血风险显著相关。接受APT治疗的患者手术需求更大(1.2%对0.4%;<0.0001),住院率更高(52.9%对37.4%;<0.0001),并且出院时其临床状况更严重(根据一维定量五点数字量表上的出院代码值评估)(=0.013)。两组因头部创伤返回急诊科复诊的频率没有差异。接受APT治疗且发生MHT的患者的出血风险并不高于对照组。然而,接受APT治疗的患者的临床状况更严重,包括因ICH监测住院和进行颅脑神经外科干预。