Vassy Jason L, Gaziano J Michael, Green Robert C, Ferguson Ryan E, Advani Sanjay, Miller Stephen J, Chun Sojeong, Hage Anthony K, Seo Soo-Ji, Majahalme Nilla, MacMullen Lauren, Zimolzak Andrew J, Brunette Charles A
VA Boston Healthcare System, Boston, Massachusetts.
Department of Medicine, Harvard Medical School, Boston, Massachusetts.
JAMA Netw Open. 2020 Dec 1;3(12):e2027092. doi: 10.1001/jamanetworkopen.2020.27092.
Nonadherence to statin guidelines is common. The solute carrier organic anion transporter family member 1B1 (SLCO1B1) genotype is associated with simvastatin myopathy risk and is proposed for clinical implementation. The unintended harms of using pharmacogenetic information to guide pharmacotherapy remain a concern for some stakeholders.
To determine the impact of delivering SLCO1B1 pharmacogenetic results to physicians on the effectiveness of atherosclerotic cardiovascular disease (ASCVD) prevention (measured by low-density lipoprotein cholesterol [LDL-C] levels) and concordance with prescribing guidelines for statin safety and effectiveness.
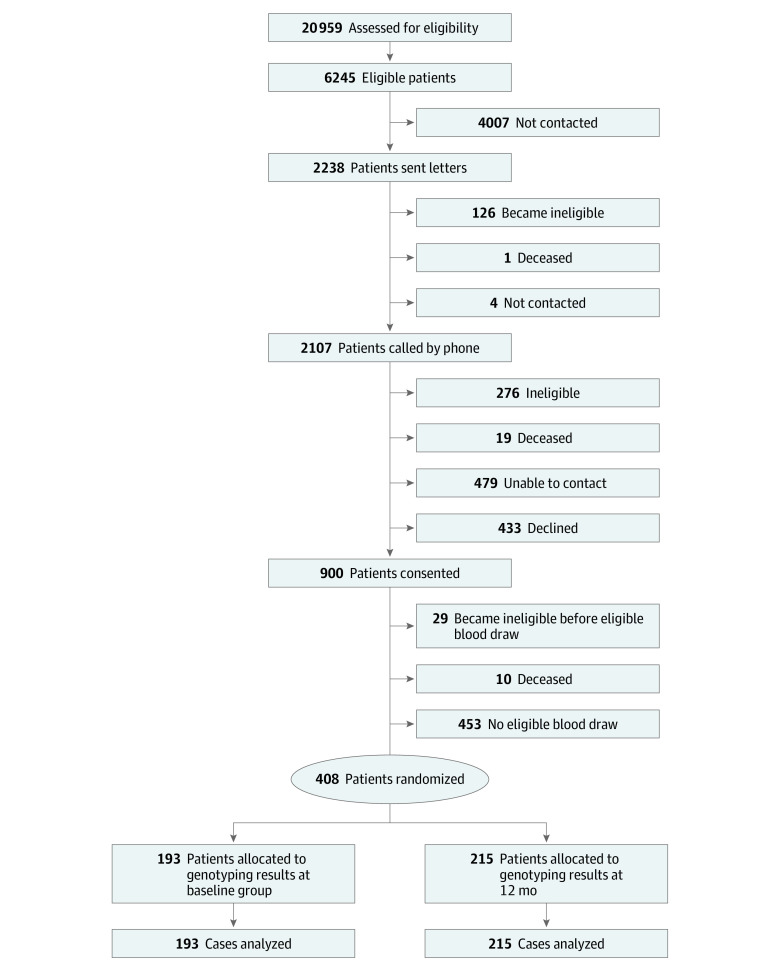
DESIGN, SETTING, AND PARTICIPANTS: This randomized clinical trial was performed from December 2015 to July 2019 at 8 primary care practices in the Veterans Affairs Boston Healthcare System. Participants included statin-naive patients with elevated ASCVD risk. Data analysis was performed from October 2019 to September 2020.
SLCO1B1 genotyping and results reporting to primary care physicians at baseline (intervention group) vs after 1 year (control group).
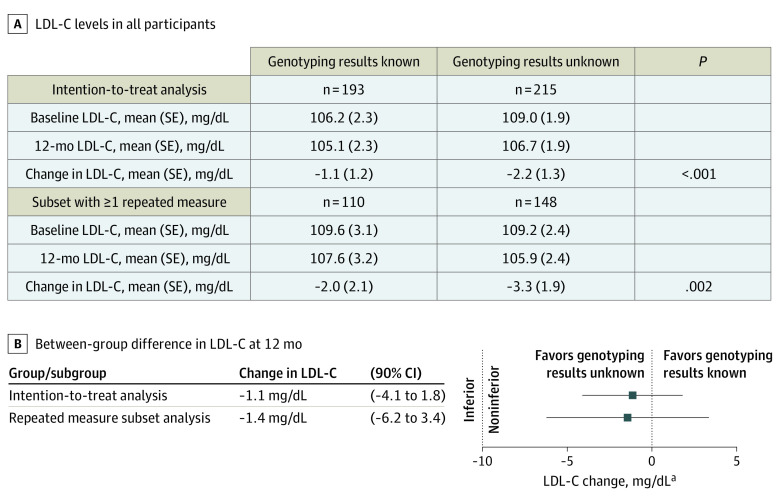
The primary outcome was the 1-year change in LDL-C level. The secondary outcomes were 1-year concordance with American College of Cardiology-American Heart Association and Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines for statin therapy and statin-associated muscle symptoms (SAMS).
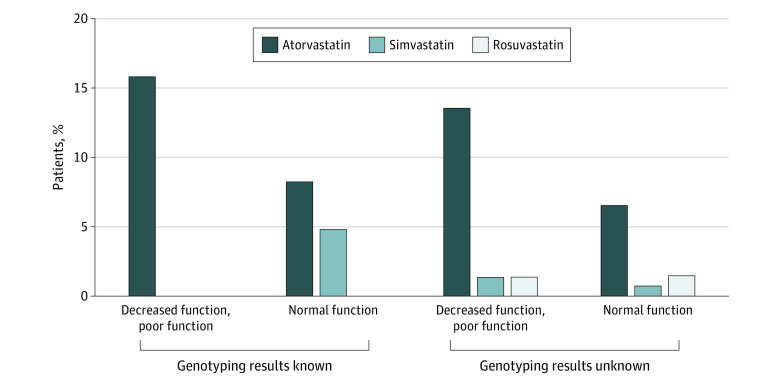
Among 408 patients (mean [SD] age, 64.1 [7.8] years; 25 women [6.1%]), 193 were randomized to the intervention group and 215 were randomized to the control group. Overall, 120 participants (29%) had a SLCO1B1 genotype indicating increased simvastatin myopathy risk. Physicians offered statin therapy to 65 participants (33.7%) in the intervention group and 69 participants (32.1%) in the control group. Compared with patients whose physicians did not know their SLCO1B1 results at baseline, patients whose physicians received the results had noninferior reductions in LDL-C at 12 months (mean [SE] change in LDL-C, -1.1 [1.2] mg/dL in the intervention group and -2.2 [1.3] mg/dL in the control group; difference, -1.1 mg/dL; 90% CI, -4.1 to 1.8 mg/dL; P < .001 for noninferiority margin of 10 mg/dL). The proportion of patients with American College of Cardiology-American Heart Association guideline-concordant statin prescriptions in the intervention group was noninferior to that in the control group (12 patients [6.2%] vs 14 patients [6.5%]; difference, -0.003; 90% CI, -0.038 to 0.032; P < .001 for noninferiority margin of 15%). All patients in both groups were concordant with CPIC guidelines for safe statin prescribing. Physicians documented 2 and 3 cases of SAMS in the intervention and control groups, respectively, none of which was associated with a CPIC guideline-discordant prescription. Among patients with a decreased or poor SLCO1B1 transporter function genotype, simvastatin was prescribed to 1 patient in the control group but none in the intervention group.
Clinical testing and reporting of SLCO1B1 results for statin myopathy risk did not result in poorer ASCVD prevention in a routine primary care setting and may have been associated with physicians avoiding simvastatin prescriptions for patients at genetic risk for SAMS. Such an absence of harm should reassure stakeholders contemplating the clinical use of available pharmacogenetic results.
ClinicalTrials.gov Identifier: NCT02871934.
不遵循他汀类药物治疗指南的情况很常见。溶质载体有机阴离子转运体家族成员1B1(SLCO1B1)基因型与辛伐他汀肌病风险相关,并建议用于临床实践。对一些利益相关者来说,利用药物遗传学信息指导药物治疗的意外危害仍然令人担忧。
确定向医生提供SLCO1B1药物遗传学检测结果对动脉粥样硬化性心血管疾病(ASCVD)预防效果(通过低密度脂蛋白胆固醇[LDL-C]水平衡量)以及与他汀类药物安全性和有效性处方指南的一致性的影响。
设计、地点和参与者:这项随机临床试验于2015年12月至2019年7月在波士顿退伍军人事务医疗保健系统的8家初级保健机构进行。参与者包括ASCVD风险升高且未服用过他汀类药物的患者。数据分析于2019年10月至2020年9月进行。
在基线时对初级保健医生进行SLCO1B1基因分型并报告结果(干预组),对照组在1年后进行。
主要结局是LDL-C水平的1年变化。次要结局是与美国心脏病学会-美国心脏协会以及临床药物遗传学实施联盟(CPIC)他汀类药物治疗指南的1年一致性,以及他汀类药物相关肌肉症状(SAMS)。
在408名患者中(平均[标准差]年龄为64.1[7.8]岁;25名女性[6.1%]),193名被随机分配到干预组,215名被随机分配到对照组。总体而言,120名参与者(29%)的SLCO1B1基因型表明辛伐他汀肌病风险增加。干预组65名参与者(33.7%)和对照组69名参与者(32.1%)的医生提供了他汀类药物治疗。与基线时医生不知道其SLCO1B1结果的患者相比,医生收到结果的患者在12个月时LDL-C降低程度不劣于对照组(干预组LDL-C的平均[标准误]变化为-1.1[1.2]mg/dL,对照组为-2.2[1.3]mg/dL;差异为-1.1mg/dL;90%置信区间为-4.1至1.8mg/dL;非劣效性界值为10mg/dL时,P<0.)。干预组符合美国心脏病学会-美国心脏协会指南的他汀类药物处方患者比例不劣于对照组(12例患者[6.2%]对14例患者[6.5%];差异为-0.003;90%置信区间为-0.038至0.032;非劣效性界值为15%时,P<0.)。两组所有患者均符合CPIC安全他汀类药物处方指南。干预组和对照组医生分别记录了2例和3例SAMS病例,均与不符合CPIC指南的处方无关。在SLCO1B1转运蛋白功能基因型降低或较差的患者中,对照组有1例患者使用了辛伐他汀,干预组无患者使用。
在常规初级保健环境中,对他汀类肌病风险进行SLCO1B1结果的临床检测和报告并未导致ASCVD预防效果变差,并且可能与医生避免为有SAMS遗传风险的患者开具辛伐他汀处方有关。这种无害性应能让考虑临床使用现有药物遗传学检测结果的利益相关者放心。
ClinicalTrials.gov标识符:NCT02871934。