Park Seong Yong, Hong Min Hee, Kim Hye Ryun, Lee Chang Geol, Cho Jae Ho, Cho Byoung Chul, Kim Dae Joon
Department of Thoracic and Cardiovascular Surgery, Yonsei University College of Medicine, Seoul, Republic of Korea.
Division of Medical Oncology, Department of Internal Medicine, Yonsei Cancer Center, Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea.
J Thorac Dis. 2020 Nov;12(11):6426-6434. doi: 10.21037/jtd-20-1088.
Immune checkpoint inhibitors have been tried for several thoracic malignancies; however, their application as a neoadjuvant therapy in esophageal squamous cell carcinoma (ESCC) has not been studied. We evaluated the feasibility and safety of esophagectomy and total lymphadenectomy after neoadjuvant chemoradiation therapy with pembrolizumab.
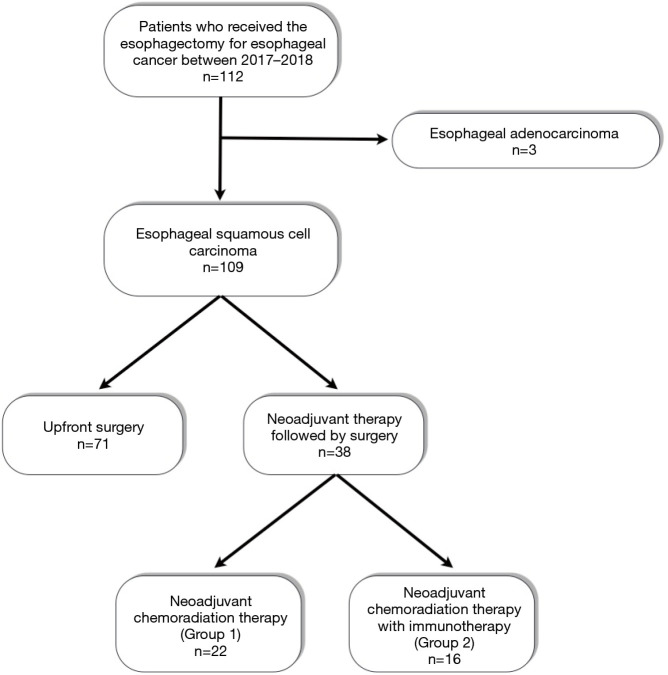
Between 2017 and 2018, 38 patients who received the neoadjuvant therapy followed by radical esophagectomy and total lymphadenectomy for ESCC were analyzed. Twenty-two patients received conventional neoadjuvant chemoradiation therapy (Group 1), and sixteen patients received neoadjuvant chemoradiation therapy with pembrolizumab in clinical trial (Group 2). Two groups were compared retrospectively.
The basic characteristics of age, clinical stage, location and methods of operation were not different between the two groups. The pathologic stages were higher in Group 2, but the difference was not statistically significant. The operative outcomes, i.e., operation time, blood loss, and numbers of dissected lymph nodes in the thorax, neck, and abdomen were comparable. Complications, including pulmonary complications and anastomotic leakage, were also comparable. The rate of recurrent laryngeal nerve palsy was also comparable between the two groups (31.8% 18.8%, P=0.469). Operative mortalities developed in 2 patients [0 2 (12.5%), P=0.171] due to acute respiratory distress syndrome (ARDS).
Radical esophagectomy for esophageal squamous cell carcinoma after neoadjuvant chemoradiation therapy with pembrolizumab may not increase the operative risk or reduce the quality of radical dissection including lymphadenectomy. The risk of ARDS after neoadjuvant neoadjuvant chemoradiation therapy with pembrolizumab has to be studied in the further analysis.
免疫检查点抑制剂已在多种胸部恶性肿瘤中进行了尝试;然而,其作为食管鳞状细胞癌(ESCC)新辅助治疗的应用尚未得到研究。我们评估了帕博利珠单抗新辅助放化疗后行食管切除术和全淋巴结清扫术的可行性和安全性。
对2017年至2018年间38例接受新辅助治疗后行ESCC根治性食管切除术和全淋巴结清扫术的患者进行分析。22例患者接受传统新辅助放化疗(第1组),16例患者在临床试验中接受帕博利珠单抗新辅助放化疗(第2组)。对两组进行回顾性比较。
两组在年龄、临床分期、病变部位和手术方式等基本特征方面无差异。第2组的病理分期较高,但差异无统计学意义。手术结果,即手术时间、失血量以及胸部、颈部和腹部清扫的淋巴结数量相当。包括肺部并发症和吻合口漏在内的并发症也相当。两组喉返神经麻痹发生率也相当(31.8%对18.8%,P = 0.469)。2例患者因急性呼吸窘迫综合征(ARDS)发生手术死亡[0对2例(12.5%),P = 0.171]。
帕博利珠单抗新辅助放化疗后行食管鳞状细胞癌根治性食管切除术可能不会增加手术风险,也不会降低包括淋巴结清扫在内的根治性切除质量。帕博利珠单抗新辅助放化疗后ARDS的风险有待进一步分析研究。