Department of Surgical Science, University of Perugia, Piazza dell' Università 1, 06100, Perugia, Italy.
Inguinal NerveWorking Group, Terni, Italy.
BMC Surg. 2020 Dec 7;20(1):319. doi: 10.1186/s12893-020-00988-1.
Nerve identification is recommended in inguinal hernia repair to reduce or avoid postoperative pain. The aim of this prospective observational study was to identify nerve prevalence and find a correlation between neuroanatomy and chronic neuropathic postoperative inguinal pain (CPIP) after 6 months.
A total of 115 patients, who underwent inguinal hernia mesh repair (Lichtenstein tension-free mesh repair) between July 2018 and January 2019, were included in this prospective observational study. The mean age and BMI respectively resulted 64 years and 25.8 with minimal inverse distribution of BMI with respect to age. Most of the hernias were direct (59.1%) and of medium dimension (47.8%). Furthermore, these patients were undergoing Dermatome Mapping Test in preoperatively and postoperatively 6 months evaluation.
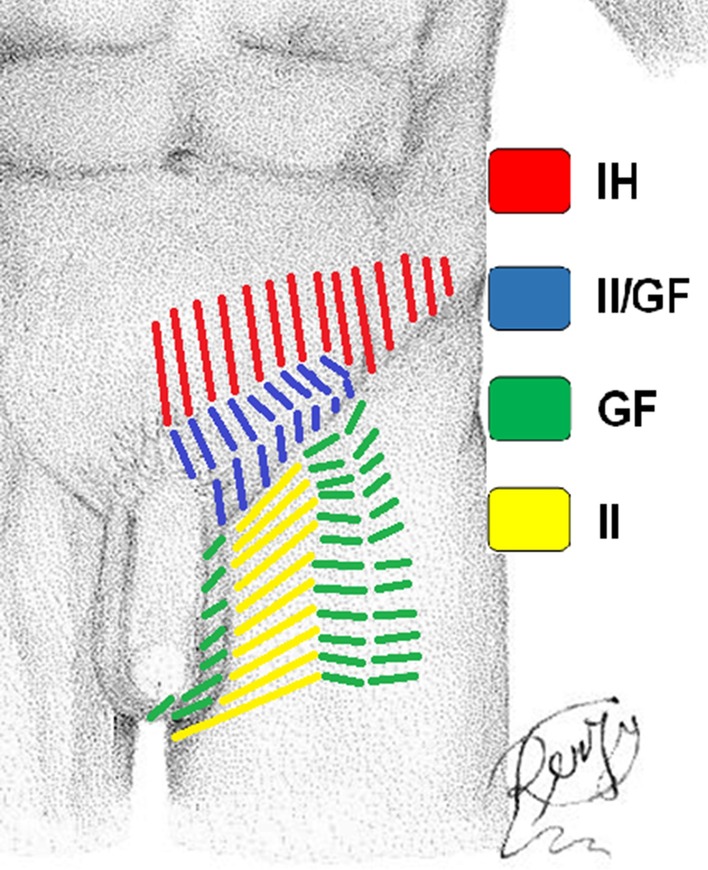
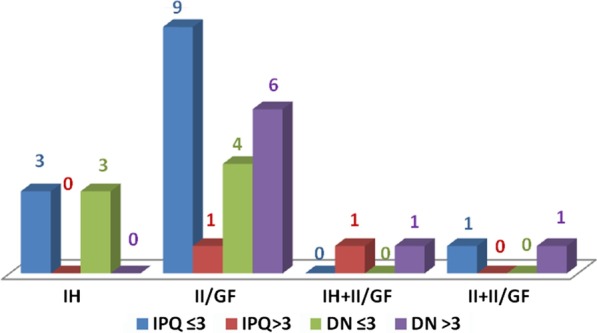
Identification rates of the iliohypogastric (IH), ilioinguinal (II) and genitofemoral (GF) nerves were 72.2%, 82.6% and 48.7% respectively. In the analysis of nerve prevalence according to BMI, the IH was statistically significant higher in patients with BMI < 25 than BMI ≥ 25 P (< 0.05). After inguinal hernia mesh repair, 8 patients (6.9%) had chronic postoperative neuropathic inguinal pain after 6 months. The CPIP prevailed at II/GF dermatome. The relation between the identification/neurectomy of the II nerve and chronic postoperative inguinal pain after 6 months was not significant (P = 0.542).
The anatomy of inguinal nerve is very heterogeneous and for this reason an accurate knowledge of these variations is needed during the open mesh repair of inguinal hernias. The new results of our analysis is the statistically significant higher IH nerve prevalence in patients with BMI < 25; probably the identification of inguinal nerve is more complex in obese patients. In the chronic postoperative inguinal pain, the II nerve may have a predominant role in determining postoperative long-term symptoms. Dermatome Mapping Test in an easy and safe method for preoperative and postoperative 6 months evaluation of groin pain. The most important evidence of our analysis is that the prevalence of chronic pain is higher when the nerves were not identified.
神经识别被推荐用于腹股沟疝修补术,以减少或避免术后疼痛。本前瞻性观察研究的目的是确定神经的发生率,并在术后 6 个月时找到神经解剖结构与慢性术后腹股沟疼痛(CPIP)之间的相关性。
本前瞻性观察研究共纳入 2018 年 7 月至 2019 年 1 月期间接受腹股沟疝网片修补术(Lichtenstein 无张力网片修补术)的 115 例患者。平均年龄和 BMI 分别为 64 岁和 25.8,BMI 与年龄呈最小反分布。大多数疝为直接疝(59.1%),中等大小(47.8%)。此外,这些患者在术前和术后 6 个月进行了皮节定位测试。
髂腹下神经(IH)、髂腹股沟神经(II)和生殖股神经(GF)的识别率分别为 72.2%、82.6%和 48.7%。根据 BMI 分析神经发生率,BMI<25 的患者 IH 显著高于 BMI≥25(P<0.05)。腹股沟疝网片修补术后,8 例(6.9%)患者在术后 6 个月出现慢性术后神经性腹股沟疼痛。CPIP 主要位于 II/GF 皮节。II 神经的识别/神经切除术与术后 6 个月慢性腹股沟疼痛之间无显著相关性(P=0.542)。
腹股沟神经解剖结构非常复杂,因此在开放式网片修补腹股沟疝时需要准确了解这些变异。我们分析的新结果是 BMI<25 的患者 IH 神经发生率显著较高;可能肥胖患者的腹股沟神经识别更复杂。在慢性术后腹股沟疼痛中,II 神经在确定术后长期症状方面可能起主要作用。皮节定位测试是一种简单、安全的方法,可用于术前和术后 6 个月的腹股沟疼痛评估。我们分析的最重要证据是,当神经未被识别时,慢性疼痛的发生率更高。