Funston Garth, Hardy Victoria, Abel Gary, Crosbie Emma J, Emery Jon, Hamilton Willie, Walter Fiona M
The Primary Care Unit, Department of Public Health and Primary Care, University of Cambridge, Cambridge CB1 8RN, UK.
University of Exeter Medical School, University of Exeter, Exeter EX1 1TX, UK.
Cancers (Basel). 2020 Dec 8;12(12):3686. doi: 10.3390/cancers12123686.
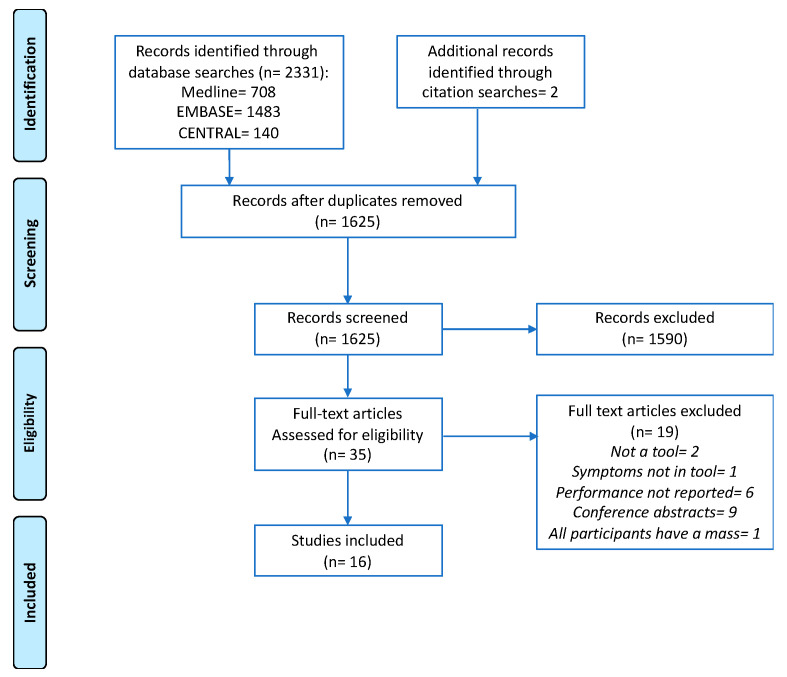
In the absence of effective ovarian cancer screening programs, most women are diagnosed following the onset of symptoms. Symptom-based tools, including symptom checklists and risk prediction models, have been developed to aid detection. The aim of this systematic review was to identify and compare the diagnostic performance of these tools. We searched MEDLINE, EMBASE and Cochrane CENTRAL, without language restriction, for relevant studies published between 1 January 2000 and 3 March 2020. We identified 1625 unique records and included 16 studies, evaluating 21 distinct tools in a range of settings. Fourteen tools included only symptoms; seven also included risk factors or blood tests. Four tools were externally validated-the Goff Symptom Index (sensitivity: 56.9-83.3%; specificity: 48.3-98.9%), a modified Goff Symptom Index (sensitivity: 71.6%; specificity: 88.5%), the Society of Gynaecologic Oncologists consensus criteria (sensitivity: 65.3-71.5%; specificity: 82.9-93.9%) and the QCancer Ovarian model (10% risk threshold-sensitivity: 64.1%; specificity: 90.1%). Study heterogeneity precluded meta-analysis. Given the moderate accuracy of several tools on external validation, they could be of use in helping to select women for ovarian cancer investigations. However, further research is needed to assess the impact of these tools on the timely detection of ovarian cancer and on patient survival.
由于缺乏有效的卵巢癌筛查项目,大多数女性在出现症状后才被诊断出来。已经开发了基于症状的工具,包括症状清单和风险预测模型,以帮助进行检测。本系统评价的目的是识别和比较这些工具的诊断性能。我们检索了MEDLINE、EMBASE和Cochrane CENTRAL,不限语言,查找2000年1月1日至2020年3月3日期间发表的相关研究。我们识别出1625条独特记录,纳入了16项研究,评估了一系列环境中的21种不同工具。14种工具仅包括症状;7种还包括风险因素或血液检测。4种工具进行了外部验证——戈夫症状指数(敏感性:56.9%-83.3%;特异性:48.3%-98.9%)、改良的戈夫症状指数(敏感性:71.6%;特异性:88.5%)、妇科肿瘤学家协会共识标准(敏感性:65.3%-71.5%;特异性:82.9%-93.9%)和QCancer卵巢模型(10%风险阈值——敏感性:64.1%;特异性:90.1%)。研究异质性妨碍了荟萃分析。鉴于几种工具在外部验证中的准确性中等,它们可用于帮助选择进行卵巢癌检查的女性。然而,需要进一步研究来评估这些工具对卵巢癌及时检测和患者生存的影响。