The Norwich School of Medicine, University of East Anglia, Norwich, Norfolk, United Kingdom.
School of Environmental Sciences, University of East Anglia, Norwich, Norfolk, United Kingdom.
Euro Surveill. 2020 Dec;25(49). doi: 10.2807/1560-7917.ES.2020.25.49.2000725.
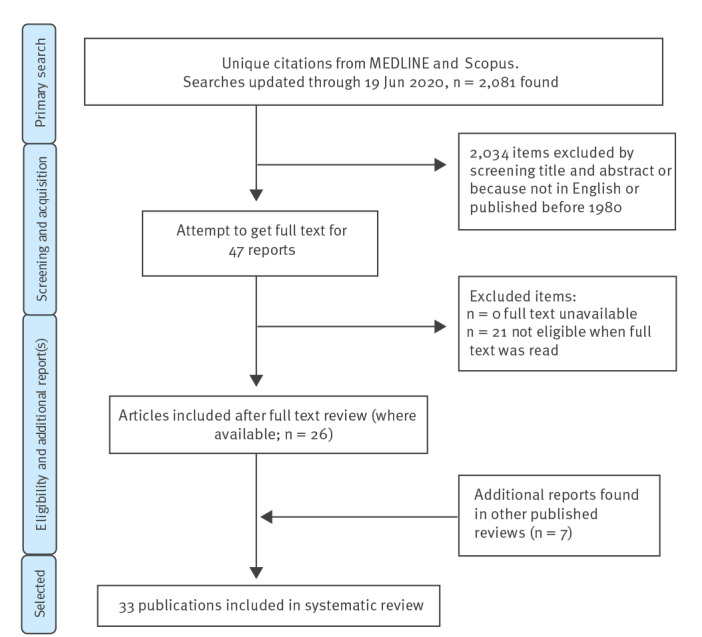
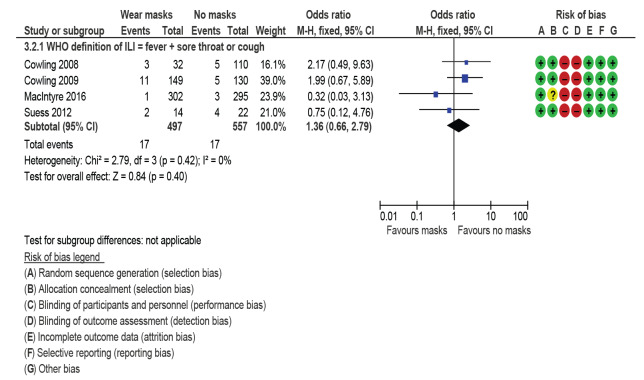
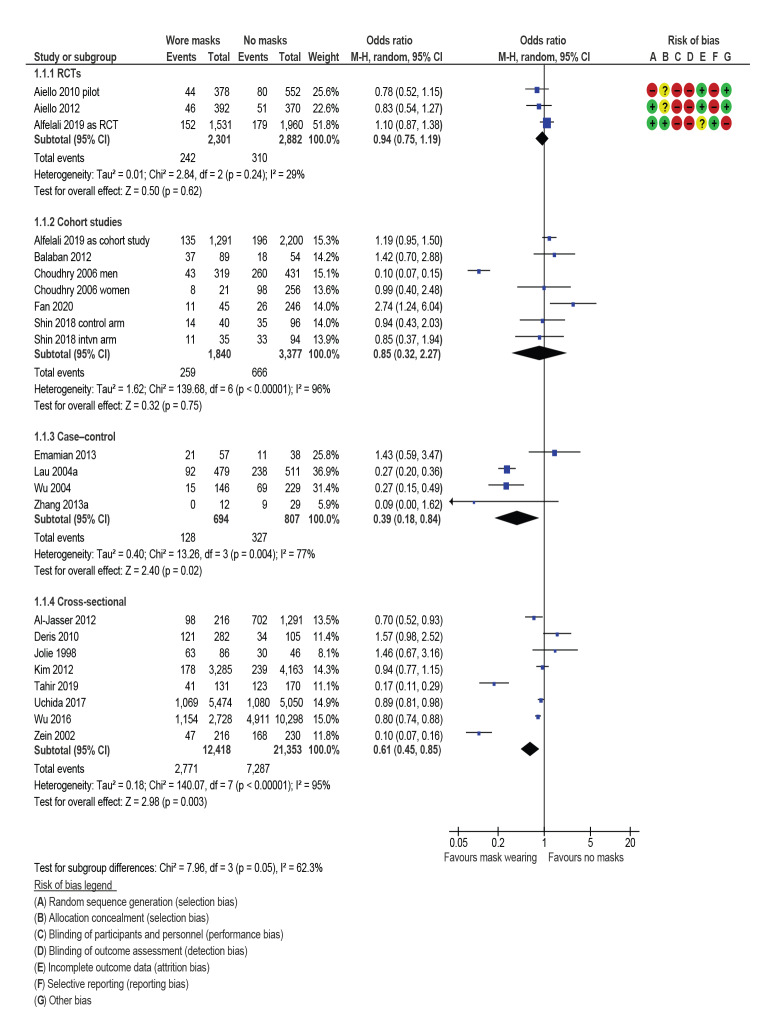
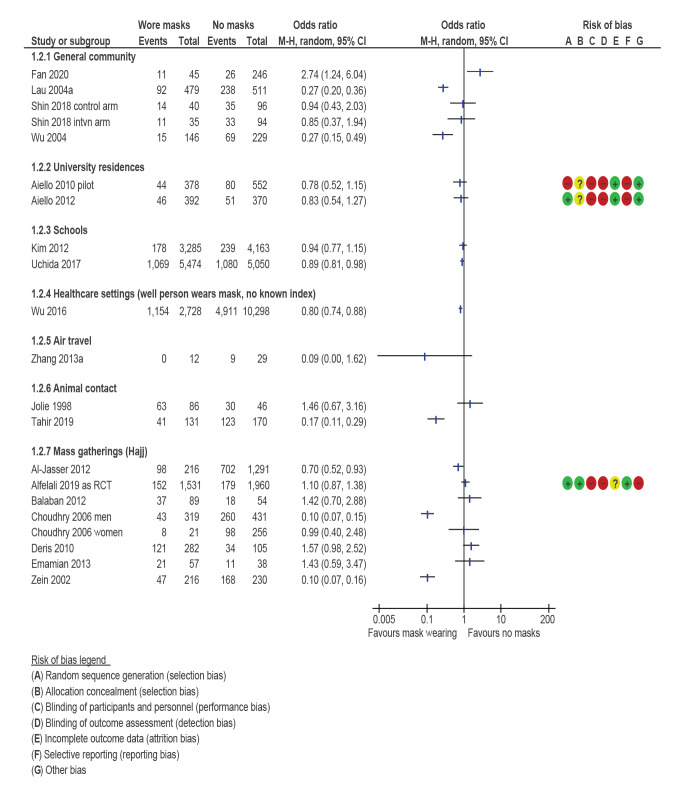
BackgroundEvidence for face-mask wearing in the community to protect against respiratory disease is unclear.AimTo assess effectiveness of wearing face masks in the community to prevent respiratory disease, and recommend improvements to this evidence base.MethodsWe systematically searched Scopus, Embase and MEDLINE for studies evaluating respiratory disease incidence after face-mask wearing (or not). Narrative synthesis and random-effects meta-analysis of attack rates for primary and secondary prevention were performed, subgrouped by design, setting, face barrier type, and who wore the mask. Preferred outcome was influenza-like illness. Grading of Recommendations, Assessment, Development and Evaluations (GRADE) quality assessment was undertaken and evidence base deficits described.Results33 studies (12 randomised control trials (RCTs)) were included. Mask wearing reduced primary infection by 6% (odds ratio (OR): 0.94; 95% CI: 0.75-1.19 for RCTs) to 61% (OR: 0.85; 95% CI: 0.32-2.27; OR: 0.39; 95% CI: 0.18-0.84 and OR: 0.61; 95% CI: 0.45-0.85 for cohort, case-control and cross-sectional studies respectively). RCTs suggested lowest secondary attack rates when both well and ill household members wore masks (OR: 0.81; 95% CI: 0.48-1.37). While RCTs might underestimate effects due to poor compliance and controls wearing masks, observational studies likely overestimate effects, as mask wearing might be associated with other risk-averse behaviours. GRADE was low or very low quality.ConclusionWearing face masks may reduce primary respiratory infection risk, probably by 6-15%. It is important to balance evidence from RCTs and observational studies when their conclusions widely differ and both are at risk of significant bias. COVID-19-specific studies are required.
社区内佩戴口罩预防呼吸道疾病的证据尚不清楚。
评估社区内佩戴口罩预防呼吸道疾病的效果,并为该证据基础提出改进建议。
我们系统地在 Scopus、Embase 和 MEDLINE 中检索了评估佩戴口罩(或不佩戴口罩)后呼吸道疾病发病率的研究。对一级和二级预防的发病率进行了叙述性综合和随机效应荟萃分析,并按设计、设置、面罩类型和佩戴口罩的人员进行了分组。首选结局是流感样疾病。采用推荐评估、制定与评价(GRADE)质量评估进行了评估,并描述了证据基础的缺陷。
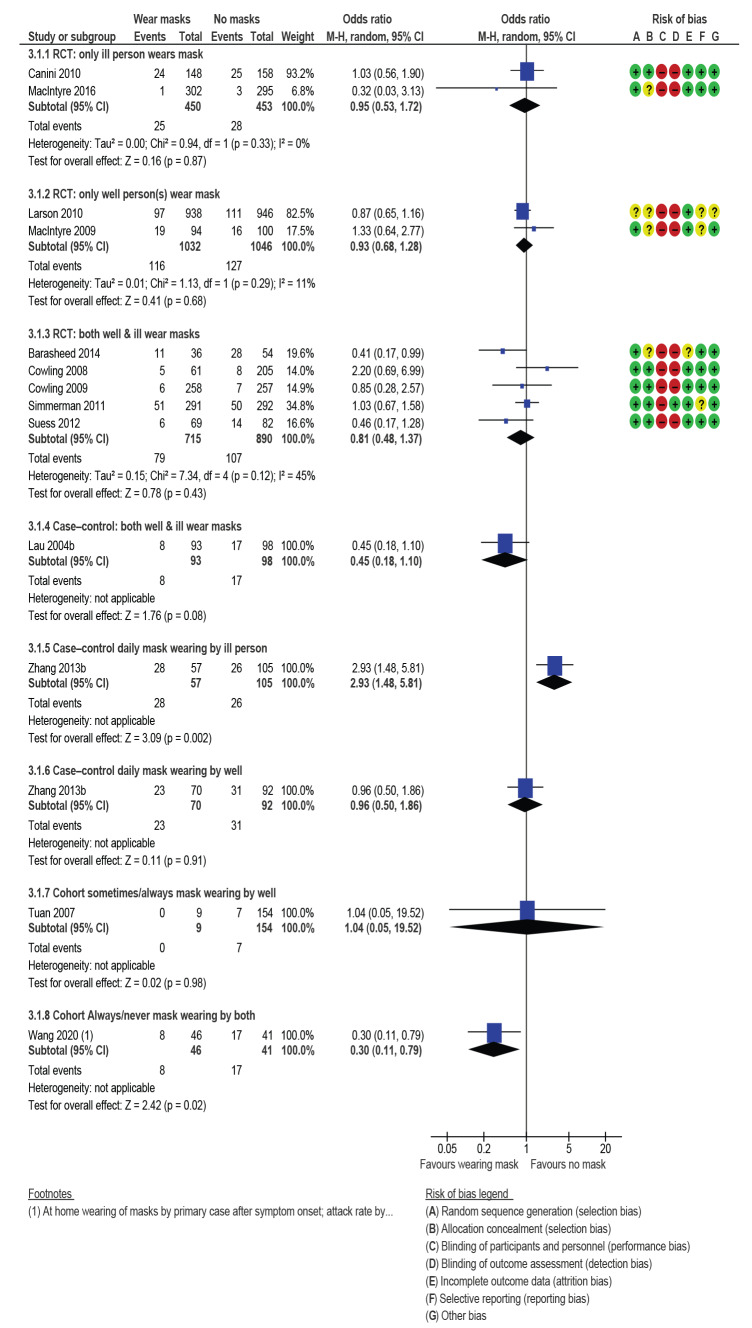
共纳入 33 项研究(12 项随机对照试验(RCT))。口罩佩戴使原发性感染减少 6%(比值比(OR):0.94;95%置信区间(CI):0.75-1.19 用于 RCT)至 61%(OR:0.85;95%CI:0.32-2.27;OR:0.39;95%CI:0.18-0.84 和 OR:0.61;95%CI:0.45-0.85 用于队列、病例对照和横断面研究)。RCT 表明,当所有健康和患病的家庭成员都佩戴口罩时,继发性感染率最低(OR:0.81;95%CI:0.48-1.37)。虽然 RCT 可能由于依从性差和对照组佩戴口罩而低估了效果,但观察性研究可能高估了效果,因为佩戴口罩可能与其他避险行为有关。GRADE 为低或极低质量。
佩戴口罩可能会降低原发性呼吸道感染的风险,可能降低 6-15%。当 RCT 和观察性研究的结论差异很大且两者都存在严重偏倚风险时,平衡两者的证据非常重要。需要进行针对 COVID-19 的特定研究。