Kamran Sultan M, Mirza Zill-E-Humayun, Moeed Hussain Abdul, Naseem Arshad, Hussain Maryam, Fazal Imran, Saeed Farrukh, Alamgir Wasim, Saleem Salman, Riaz Sidra
Pulmonology, Pak Emirates Military Hospital, Rawalpindi, PAK.
Internal Medicine, Pak Emirates Military Hospital, Rawalpindi, PAK.
Cureus. 2020 Nov 7;12(11):e11368. doi: 10.7759/cureus.11368.
Coronavirus disease 2019 (COVID-19) is a novel infectious disease of multi-system involvement with significant pulmonary manifestations. So far, many prognostic models have been introduced to guide treatment and resource management. However, data on the impact of measurable respiratory parameters associated with the disease are scarce.
To demonstrate the role of Comorbidity-Age-Lymphocyte count-Lactate dehydrogenase (CALL) score and to introduce Respiratory Assessment Scoring (RAS) model in predicting disease progression and mortality in COVID-19.
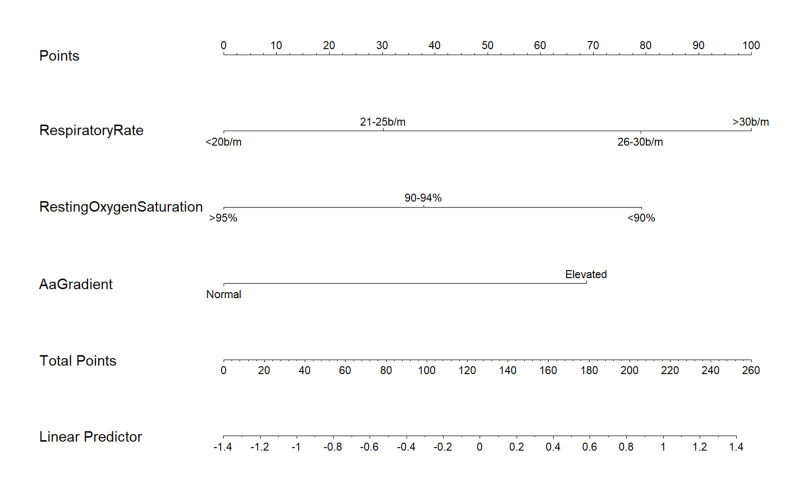
Data of 252 confirmed COVID-19 patients were collected at Pak Emirates Military Hospital (PEMH) from 10th April 2020 to 31st August 2020. The CALL score and proposed factors of RAS model, namely respiratory rate, oxygen saturation at rest, alveolar arterial gradient and minimal exercise desaturation test, were calculated on the day of admission. Progression of disease was defined and correlated with measured variables. Univariate and multivariate Cox regression analysis for each variable, its hazard ratio (HR) and 95% confidence interval (CI) were calculated, and a nomogram was made using the high-risk respiratory parameters to establish the RAS model.
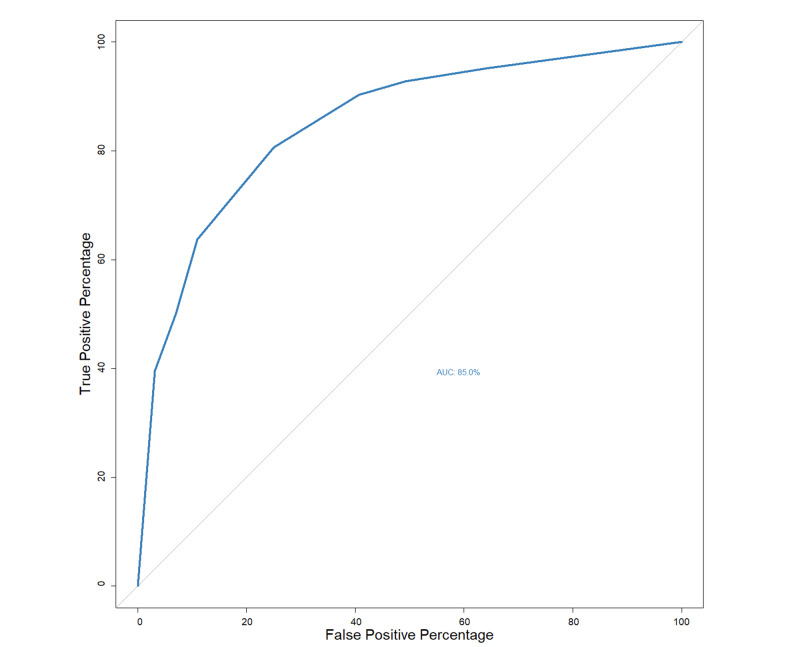
Progression of disease and death was observed in 124 (49.2%) and 49 (19.4%) patients, respectively. Presence of more than 50% of chest infiltrates was significantly associated with worsening disease and death (p-value <0.001). Death was observed in 100% of patients who had critical disease category on presentation. Regression analysis showed that the presence of comorbidity (n: 180), in contrast to other variables of CALL score, was not a good prognosticator of disease severity (p-value: 0.565). Nonetheless, the CALL model itself was validated to be a reliable prognostic indicator of disease progression and mortality. Some 10 feet oxygen desaturation test (HR: 0.99, 95%CI: 0.95-1.04, p--value: 0.706) was not a powerful predictor of the progression of disease. However, respiratory rate of more than 30 breaths/minute (b/m) (HR: 3.03, 95%CI: 1.77-5.19), resting oxygen saturation of less than 90% (HR: 2.41, 95%CI: 1.15-5.06), and an elevated alveolar-arterial oxygen gradient (HR: 2.14, 95%CI: 1.04-4.39) were considered statistically significant high-risk predictors of disease progression and death, in the formed RAS model. The model resulted in 85% (95%CI: 80%-89%) of area under the receiver operating characteristic curve (AUROC), with substantial positive (76%, 95%CI: 68%-83%) and negative predictive values (80%, 95%CI: 73%-87%) for a cutoff value of seven. Patients with higher CALL and RAS scores also resulted in higher mortality.
CALL and RAS scores were strongly associated with progression and mortality in patients with COVID-19.
2019冠状病毒病(COVID-19)是一种累及多系统的新型传染病,有显著的肺部表现。到目前为止,已经引入了许多预后模型来指导治疗和资源管理。然而,关于与该疾病相关的可测量呼吸参数影响的数据却很稀少。
证明合并症-年龄-淋巴细胞计数-乳酸脱氢酶(CALL)评分的作用,并介绍呼吸评估评分(RAS)模型在预测COVID-19疾病进展和死亡率方面的作用。
于2020年4月10日至2020年8月31日在巴基斯坦阿联酋军事医院(PEMH)收集了252例确诊COVID-19患者的数据。入院当天计算CALL评分以及RAS模型的相关因素,即呼吸频率、静息时氧饱和度、肺泡动脉氧分压差和极轻微运动时氧饱和度下降试验。定义疾病进展并将其与测量变量相关联。计算每个变量的单因素和多因素Cox回归分析、其风险比(HR)和95%置信区间(CI),并使用高风险呼吸参数制作列线图以建立RAS模型。
分别有124例(49.2%)和49例(19.4%)患者出现疾病进展和死亡。胸部浸润超过50%与疾病恶化和死亡显著相关(p值<0.001)。就诊时为危重型疾病类别的患者死亡率为100%。回归分析表明,与CALL评分的其他变量相比,合并症(n:180)的存在并非疾病严重程度的良好预后指标(p值:0.565)。尽管如此,CALL模型本身被证实是疾病进展和死亡率的可靠预后指标。约10英尺氧饱和度下降试验(HR:0.99,95%CI:0.95-1.04,p值:0.706)并非疾病进展的有力预测指标。然而,呼吸频率超过30次/分钟(b/m)(HR:3.03,95%CI:1.77-5.19)、静息氧饱和度低于90%(HR:2.41,95%CI:1.15-5.06)以及肺泡动脉氧梯度升高(HR:2.14,95%CI:1.04-4.39)在形成的RAS模型中被认为是疾病进展和死亡的统计学显著高风险预测指标。该模型在受试者工作特征曲线(AUROC)下的面积为85%(95%CI:80%-89%),对于临界值为7时,具有较高的阳性预测值(76%,95%CI:68%-83%)和阴性预测值(80%,95%CI:73%-87%)。CALL和RAS评分较高的患者死亡率也更高。
CALL和RAS评分与COVID-