King Edward VIII Hospital, Durban, South Africa.
Lecturer Nelson R Mandela School of Clinical Medicine, King Edward VIII Hospital, Durban, South Africa.
BMC Emerg Med. 2022 Apr 29;22(1):68. doi: 10.1186/s12873-022-00631-7.
COVID-19 remains a major healthcare concern. Vital signs are routinely measured on admission and may provide an early, cost-effective indicator of outcome - more so in developing countries where such data is scarce. We sought to describe the association between six routinely measured admission vital signs and COVID-19 mortality, and secondarily to derive potential applications for resource-limited settings.
Retrospective analysis of consecutive patients admitted to King Edward VIII Hospital, South Africa, with COVID-19 during June-September 2020 was undertaken. The sample was subdivided into survivors and non-survivors and comparisons made in terms of demographics and admission vital signs. Univariate and multivariate analysis of predictor variables identified associations with in-hospital mortality, with the resulting multivariate regression model evaluated for its predictive ability with receiver operating characteristic (ROC) curve analysis.
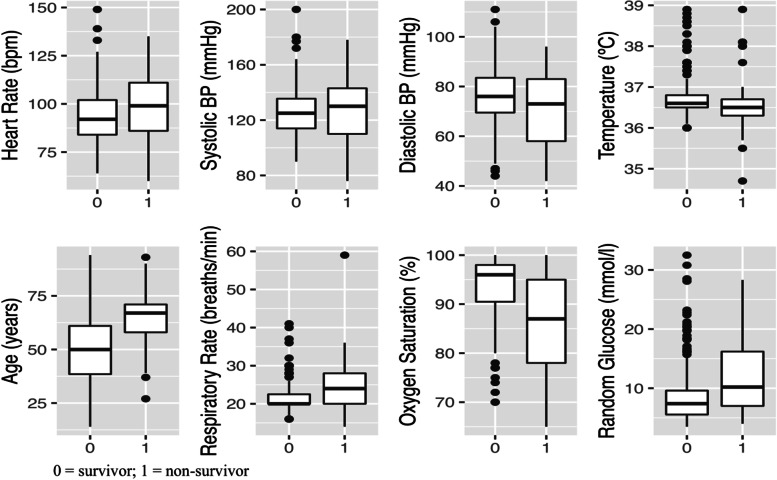
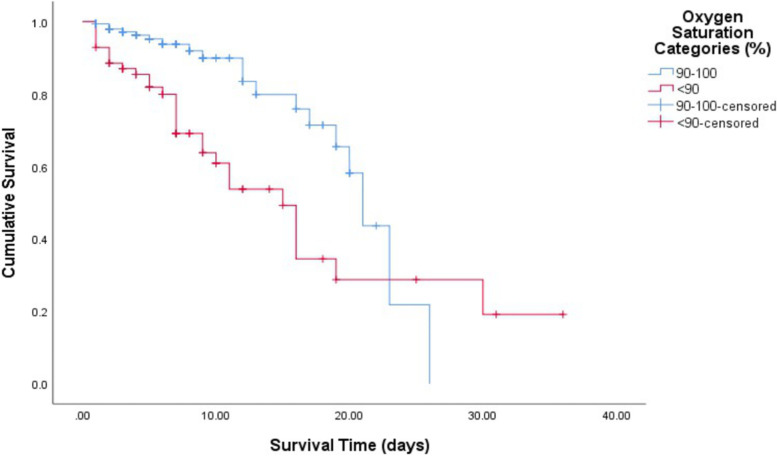
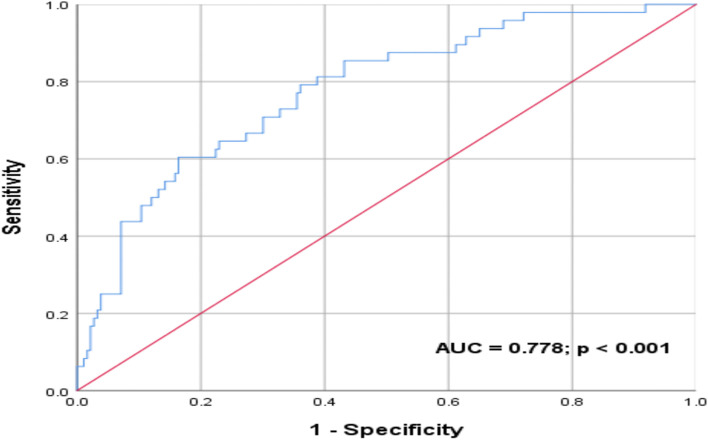
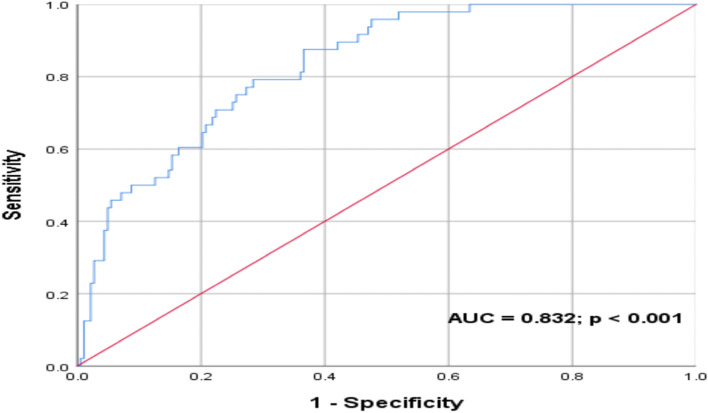
The 236 participants enrolled comprised 153(77.54%) survivors and 53(22.46%) non-survivors. Most participants were Black African(87.71%) and female(59.75%) with a mean age of 53.08(16.96) years. The non-survivor group demonstrated a significantly lower median/mean for admission oxygen saturation (%) [87(78-95) vs. 96(90-98)] and diastolic BP (mmHg) [70.79(14.66) vs. 76.3(12.07)], and higher median for admission respiratory rate (breaths/minute) [24(20-28) vs. 20(20-23)] and glucose (mmol/l) [10.2(6.95-16.25) vs. 7.4(5.5-9.8)]. Age, oxygen saturation, respiratory rate, glucose and diastolic BP were found to be significantly associated with mortality on univariate analysis. A log rank test revealed significantly lower survival rates in patients with an admission oxygen saturation < 90% compared with ≥90% (p = 0.001). Multivariate logistic regression revealed a significant relationship between age and oxygen saturation with in-hospital mortality (OR 1.047; 95% CI 1.016-1.080; p = 0.003 and OR 0.922; 95% CI 0.880-0.965; p = 0.001 respectively). A ROC curve analysis generated an area under the curve (AUC) of 0.778 (p < 0.001) when evaluating the predictive ability of oxygen saturation, respiratory rate, glucose and diastolic BP for in-hospital death. This improved to an AUC of 0.832 (p < 0.001) with the inclusion of age.
A multivariate regression model comprising admission oxygen saturation, respiratory rate, glucose and diastolic BP (with/without age) demonstrated promising predictive capacity, and may provide a cost-effective means for early prognostication of patients admitted with COVID-19 in resource-limited settings.
COVID-19 仍然是一个主要的医疗保健问题。生命体征通常在入院时进行测量,可能是一种早期、具有成本效益的预后指标,在资源匮乏的国家尤其如此,因为这些国家的数据稀缺。我们试图描述六种常规测量的入院生命体征与 COVID-19 死亡率之间的关联,并次要地为资源有限的环境推导出潜在的应用。
对 2020 年 6 月至 9 月期间在南非爱德华八世国王医院因 COVID-19 入院的连续患者进行回顾性分析。该样本分为幸存者和非幸存者,并在人口统计学和入院生命体征方面进行了比较。单变量和多变量分析预测变量确定了与院内死亡率的关联,使用接收者操作特征 (ROC) 曲线分析评估由此产生的多变量回归模型的预测能力。
共纳入 236 名参与者,其中 153 名(77.54%)为幸存者,53 名(22.46%)为非幸存者。大多数参与者为黑人(87.71%)和女性(59.75%),平均年龄为 53.08(16.96)岁。非幸存者组的入院时血氧饱和度(%)中位数/平均值明显较低[87(78-95)比 96(90-98)],舒张压(mmHg)[70.79(14.66)比 76.3(12.07)],而入院时呼吸频率(次/分钟)中位数较高[24(20-28)比 20(20-23)]和血糖(mmol/L)[10.2(6.95-16.25)比 7.4(5.5-9.8)]。单变量分析发现年龄、血氧饱和度、呼吸频率、血糖和舒张压与死亡率显著相关。对数秩检验显示,入院时血氧饱和度 < 90%的患者与血氧饱和度≥90%的患者相比,生存率显著降低(p=0.001)。多变量逻辑回归显示,年龄和血氧饱和度与院内死亡率之间存在显著关系(OR 1.047;95% CI 1.016-1.080;p=0.003 和 OR 0.922;95% CI 0.880-0.965;p=0.001)。ROC 曲线分析生成的曲线下面积(AUC)为 0.778(p<0.001),用于评估血氧饱和度、呼吸频率、血糖和舒张压对院内死亡的预测能力。当包含年龄时,AUC 提高到 0.832(p<0.001)。
包含入院时血氧饱和度、呼吸频率、血糖和舒张压(有/无年龄)的多变量回归模型显示出有希望的预测能力,可能为资源有限的环境中 COVID-19 入院患者的早期预后提供一种具有成本效益的手段。