Zhang Shi, Lu Zhonghua, Wu Zongsheng, Xie Jianfeng, Yang Yi, Qiu Haibo
Jiangsu Provincial Key Laboratory of Critical Care Medicine, Department of Critical Care Medicine, School of Medicine, Nanjing Zhongda Hospital, Southeast University, Nanjing, China.
Front Med (Lausanne). 2020 Nov 27;7:598621. doi: 10.3389/fmed.2020.598621. eCollection 2020.
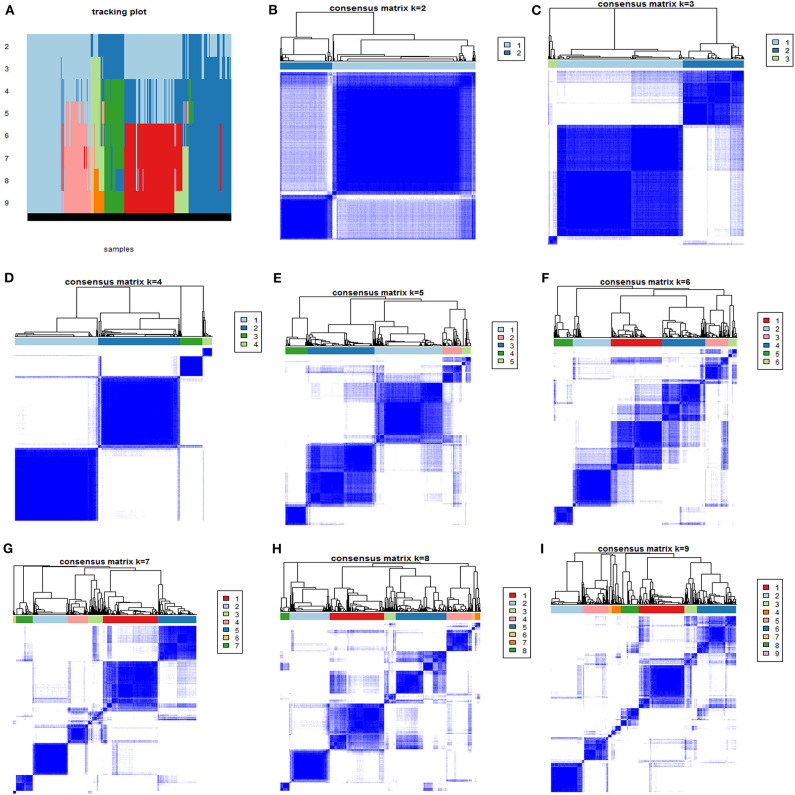
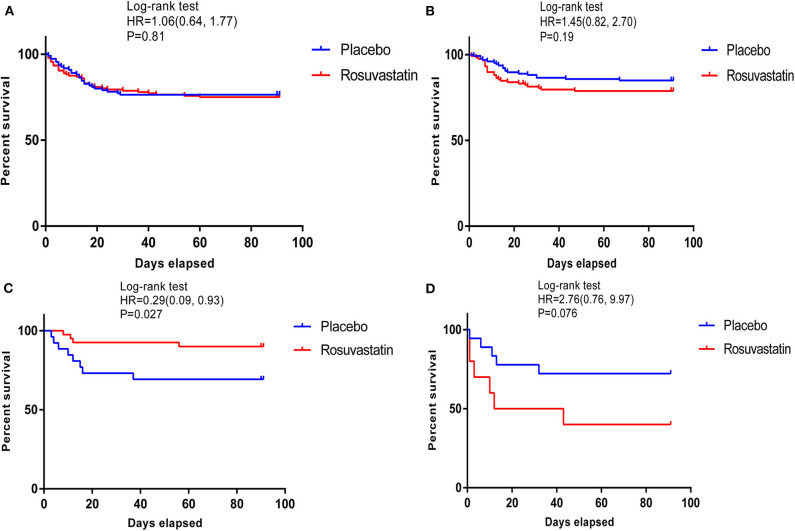
The high heterogeneity of acute respiratory distress syndrome (ARDS) contributes to paradoxical conclusions from previous investigations of rosuvastatin for ARDS. Identification of the population (phenotype) that could benefit from rosuvastatin is a novel exploration for the precise treatment. The patient population for this analysis consisted of unique patients with ARDS enrolled in the SAILS trial (rosuvastatin vs. placebo). Phenotypes were derived using consensus k-means clustering applied to routinely available clinical variables within 6 h of hospital presentation before the patients received placebo or rosuvastatin. The Kaplan-Meier statistic was used to estimate the 90-day cumulative mortality to screen for a specific population that could benefit from rosuvastatin, with a cutoff < 0.05. The derivation cohort included 585 patients with ARDS. Of the patients with the four derived phenotypes, those with phenotype 3 were classified as the "specific population who could benefit from rosuvastatin" as rosuvastatin resulted in a significant reduction in 90-day cumulative mortality from ARDS [hazard ratio (HR), 0.29; 95% confidence interval (CI), 0.09-0.93; = 0.027]. Additionally, rosuvastatin markedly improved the days free of cardiovascular failure (10.08 ± 3.79 in the rosuvastatin group vs. 7.31 ± 4.94 in the placebo group, = 0.01) and coagulation abnormalities (13.65 ± 1.33 vs. 12.15 ± 3.77, = 0.02) up to day 14 in the phenotype 3 cohort. Phenotype 3 was summarized as Platelet & Creat phenotype because these patients have a relatively higher platelet count (390.05 ± 79.43 × 10/L) and lower creatinine (1.42 ± 1.08 mg/dL) than do patients classified as other phenotypes. In addition, rosuvastatin seemed to increase 90-day mortality for patients classified as phenotype 4 (HR, 2.76; 95% CI, 0.09-9.93; = 0.076), with an adverse effect on reducing the days free of renal failure up to day 14 (4.70 ± 4.99 vs. 10.17 ± 4.69, = 0.01). Patients in phenotype 4 showed relatively severe illness in terms of baseline features, particularly renal failure, with high serum glucose. Therefore, phenotype 4 was defined as APACHE & Serum glucose phenotype. This secondary analysis of the SAILS trial identified that rosuvastatin seems to be harmful for patients classified as APACHE & Serum glucose phenotype, but benefit patients in Platelet & Creat phenotype, thus uncovering the novel value of rosuvastatin for the precise treatment of ARDS.
急性呼吸窘迫综合征(ARDS)的高度异质性导致先前关于瑞舒伐他汀治疗ARDS的研究得出相互矛盾的结论。确定可能从瑞舒伐他汀中获益的人群(表型)是精准治疗的一项新探索。本分析的患者群体包括参加SAILS试验(瑞舒伐他汀与安慰剂对照试验的ARDS患者。在患者接受安慰剂或瑞舒伐他汀之前,应用共识k均值聚类法对入院6小时内常规可得的临床变量进行分析,得出表型。采用Kaplan-Meier统计量估计90天累积死亡率,以筛选可能从瑞舒伐他汀中获益的特定人群,临界值<0.05。推导队列包括585例ARDS患者。在四种推导表型的患者中,表型3的患者被归类为“可能从瑞舒伐他汀中获益的特定人群”,因为瑞舒伐他汀使ARDS患者的90天累积死亡率显著降低[风险比(HR),0.29;95%置信区间(CI),0.09 - 0.93;P = 0.027]。此外,在表型3队列中,直至第14天,瑞舒伐他汀显著改善了无心血管衰竭天数(瑞舒伐他汀组为10.08±3.79天,安慰剂组为7.31±4.94天,P = 0.01)和凝血异常情况(13.65±1.33天对12.15±3.77天,P = 0.02)。表型3被总结为血小板与肌酐表型,因为这些患者的血小板计数(390.05±79.43×10⁹/L)相对较高,肌酐(1.42±1.08mg/dL)低于其他表型的患者。此外,瑞舒伐他汀似乎增加了表型4患者的90天死亡率(HR,2.76;95%CI,0.09 - 9.93;P = 0.076),对减少直至第14天的无肾衰竭天数有不良影响(4.70±4.99天对10.17±4.69天,P = 0.01)。表型4的患者在基线特征方面病情相对较重,尤其是肾衰竭,血糖较高。因此,表型4被定义为APACHE与血糖表型。SAILS试验的这项二次分析表明瑞舒伐他汀似乎对APACHE与血糖表型的患者有害,但对血小板与肌酐表型的患者有益,从而揭示了瑞舒伐他汀在ARDS精准治疗中的新价值。