Depinoy Thibaud, Saraux Alain, Pers Jacques-Olivier, Boisramé Sylvie, Cornec Divi, Marhadour Thierry, Guellec Dewi, Devauchelle-Pensec Valérie, Bressollette Luc, Jousse-Joulin Sandrine
Rheumatology Department, CHU de Brest, Brest, France.
UMR1227, Lymphocytes B Et Autoimmunité, Univ Brest, INSERM, LabEx IGO, Brest, France.
Rheumatol Ther. 2021 Mar;8(1):219-231. doi: 10.1007/s40744-020-00263-y. Epub 2020 Dec 17.
Oral administration of pilocarpine enhances salivary flow in sicca patients but its effect upstream on ultrasound (US) of salivary glands (SG) and downstream on periodontium remain unknown.
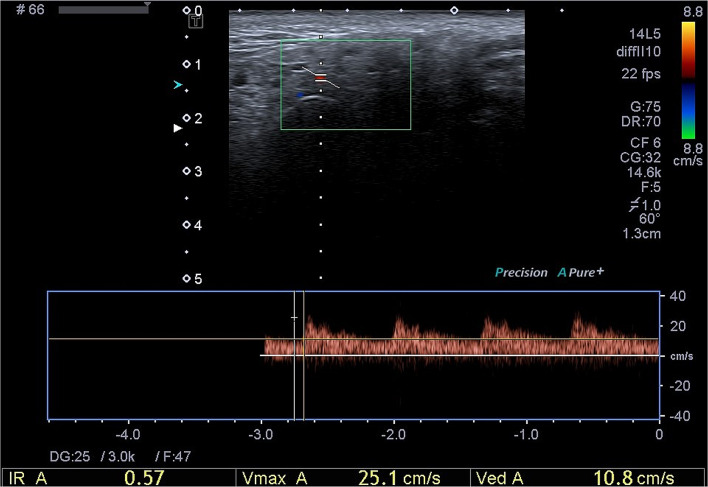
Sicca patients were prospectively included. Echostructural and vascularization of SG were assessed using B mode and pulsed Doppler (USPD). Vascularization of SG was measured using resistive index (RI) before and after stimulation by lemon juice. Echostructure (measure of glandular length in cm, evaluation of parotid and submandibular glands parenchymal abnormalities) was assessed at baseline (M0) and after 3 months (M3) of treatment with pilocarpine. A dental consultation was performed at M0 and M3 to evaluate changes in unstimulated salivary flow (USSF), stimulated salivary flow (SSF), and periodontal parameters such as modified gingival index (Lobene), plaque index (Silness), bleeding index, pocket depth, and pH.
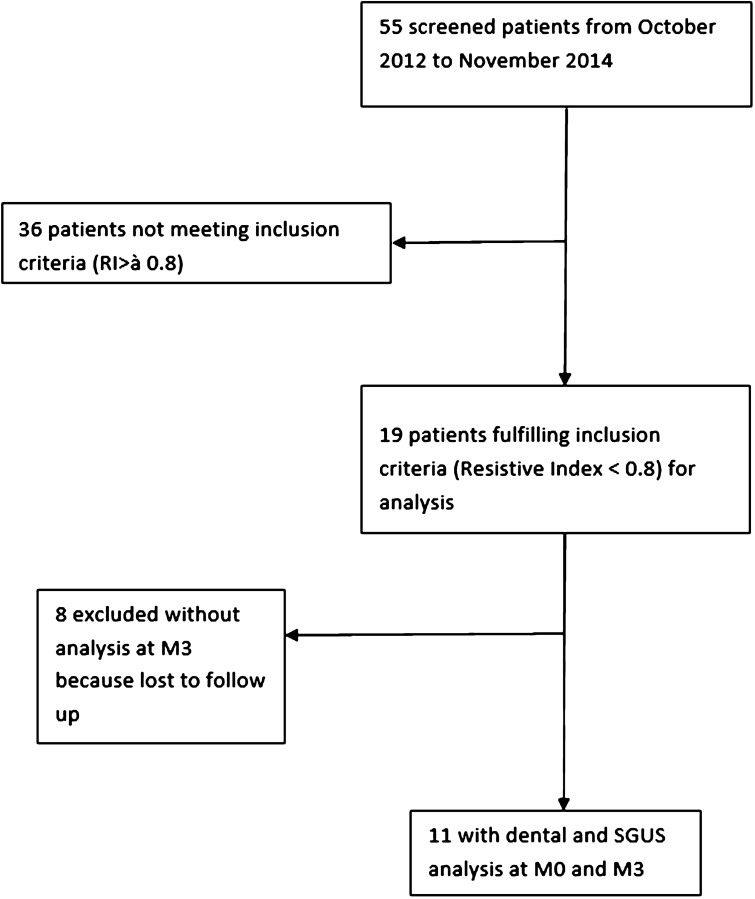
Nineteen patients were included but only 11 received pilocarpine treatment for 3 months, as six stopped pilocarpine due to side effects and two were excluded for other causes. Among the 11 patients who completed the 3-month follow-up, five had primary Sjögren's syndrome according to the American-European's classification criteria. As expected, statistical differences were found concerning SSF (p = 0.018) and USSF (p = 0.027) between M0 and M3 while no statistical change in both SG echostructure and vascularization or periodontal evaluation was shown.
Pilocarpine improved SSF and USSF measurements in sicca syndrome but no ultrasonography of major salivary glands (SGUS) structural and vascular changes were detected as well as periodontal evaluation.
口服毛果芸香碱可增加干燥综合征患者的唾液流量,但其对唾液腺超声(US)的上游影响以及对牙周组织的下游影响尚不清楚。
前瞻性纳入干燥综合征患者。使用B模式和脉冲多普勒(USPD)评估唾液腺的回声结构和血管化。在柠檬汁刺激前后,使用阻力指数(RI)测量唾液腺的血管化。在基线(M0)和毛果芸香碱治疗3个月后(M3)评估回声结构(以厘米为单位测量腺体长度,评估腮腺和颌下腺实质异常)。在M0和M3进行牙科检查,以评估未刺激唾液流量(USSF)、刺激唾液流量(SSF)以及牙周参数(如改良牙龈指数(Lobene)、菌斑指数(Silness)、出血指数、牙周袋深度和pH值)的变化。
纳入19例患者,但只有其中11例接受了3个月的毛果芸香碱治疗,6例因副作用停止使用毛果芸香碱,2例因其他原因被排除。在完成3个月随访的11例患者中,根据欧美分类标准,5例患有原发性干燥综合征。正如预期的那样,M0和M3之间在SSF(p = 0.018)和USSF(p = 0.027)方面存在统计学差异,而唾液腺回声结构和血管化或牙周评估均未显示出统计学变化。
毛果芸香碱改善了干燥综合征患者的SSF和USSF测量值,但未检测到主要唾液腺超声检查(SGUS)的结构和血管变化以及牙周评估结果。