University of Health Sciences, Haseki Training and Research Hospital, Department of Emergency Medicine, Istanbul, Turkey.
University of Health Sciences, Haseki Training and Research Hospital, Department of Cardiology, Istanbul, Turkey.
Am J Emerg Med. 2021 Feb;40:41-46. doi: 10.1016/j.ajem.2020.12.014. Epub 2020 Dec 11.
We investigated the efficacy and safety of hydroxychloroquine for empirical treatment of outpatients with confirmed COVID-19.
In this prospective, single-center study, we enrolled ambulatory outpatients with COVID-19 confirmed by a molecular method who received hydroxychloroquine. The patients were divided into low- and moderate-risk groups based on the Tisdale risk score for drug-associated QT prolongation, and the QT interval was corrected for heart rate using the Bazett formula (QTc). The QTc interval was measured by electrocardiography both pretreatment (QTc1) and 4 h after the administration of hydroxychloroquine (QTc2). The difference between the QTc1 and QTc2 intervals was defined as the ΔQTc. The QTc1 and QTc2 intervals and ΔQTc values were compared between the two risk groups.
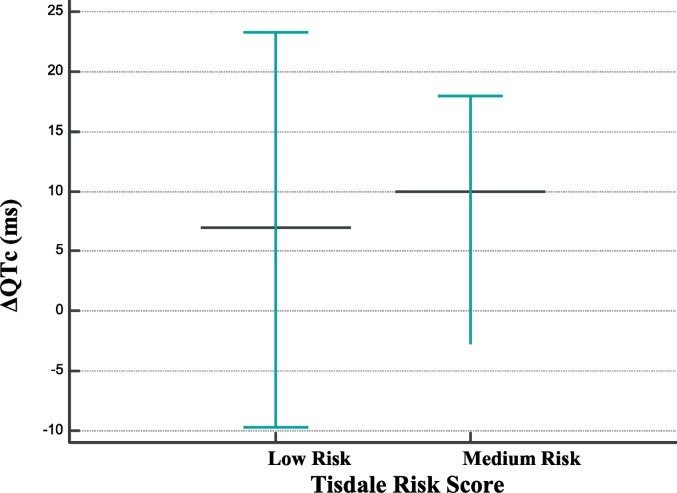
The median and interquartile range (IQR) age of the patients was 47.0 (36.2-62) years, and there were 78 men and 74 women. The median (IQR) QTc1 interval lengthened from 425.0 (407.2-425.0) to 430.0 (QTc2; 412.0-443.0) milliseconds (ms). However, this was not considered an increased risk of ventricular tachycardia associated with a prolonged QTc interval requiring drug discontinuation, because none of the patients had a ΔQTc of >60 ms or a QTc2 of >500 ms. Moreover, the median (quartiles; minimum-maximum) ΔQTc value was higher in patients in the moderate-risk group than those in the low-risk group (10.0 [-4.0-18.0; -75.0-51.0] vs. 7.0 [-10.5-23.5; -53.0-59.0 ms]) (p = 0.996). Clinical improvement was noted in 91.4% of the patients, the exceptions being 13 patients who presented with non-serious adverse drug reactions or who had severe COVID-19 and were hospitalized. Adverse effects related to hydroxychloroquine were non-serious and occurred in 52.8% (n = 80) of the patients.
Our findings show that hydroxychloroquine is safe for COVID-19 and not associated with a risk of ventricular arrhythmia due to drug-induced QTc interval prolongation. Additionally, hydroxychloroquine was well tolerated, and there were no drug-related non-serious adverse events leading to treatment discontinuation in the majority of patients who were stable and did not require hospitalization.
我们旨在研究羟氯喹(HCQ)在门诊确诊 COVID-19 患者中的疗效和安全性。
在这项前瞻性单中心研究中,我们招募了经分子方法确诊为 COVID-19 的门诊患者,他们接受了 HCQ 治疗。根据 Tisdale 药物相关 QT 延长风险评分,将患者分为低危和中危组,并用 Bazett 公式(QTc)校正心率的 QT 间期(QTc)。在服用 HCQ 前(QTc1)和 4 小时后(QTc2)通过心电图测量 QT 间期。QTc1 与 QTc2 之间的差值定义为 ΔQTc。比较两组的 QTc1 和 QTc2 间隔和 ΔQTc 值。
患者的中位和四分位距(IQR)年龄为 47.0(36.2-62)岁,其中男性 78 人,女性 74 人。中位(IQR)QTc1 间期从 425.0(407.2-425.0)延长至 430.0(QTc2;412.0-443.0)毫秒(ms)。然而,这并不被认为是与 QTc 延长相关的室性心动过速风险增加,需要停止用药,因为没有患者的 ΔQTc>60ms 或 QTc2>500ms。此外,与低危组相比,中危组的患者的中位(四分位数;最小值-最大值)ΔQTc 值更高(10.0[-4.0-18.0;-75.0-51.0]与 7.0[-10.5-23.5;-53.0-59.0ms])(p=0.996)。91.4%的患者临床改善,13 名患者除外,他们出现非严重药物不良反应或患有严重 COVID-19 而住院。与羟氯喹相关的不良反应不严重,发生在 52.8%(n=80)的患者中。
我们的研究结果表明,羟氯喹治疗 COVID-19 是安全的,不会导致因药物引起的 QT 间期延长而发生室性心律失常的风险。此外,羟氯喹的耐受性良好,大多数稳定且无需住院的患者未因药物相关的非严重不良事件而停药。