Institute D'Or for Research and Teaching, Rio de Janeiro, Brazil.
Victoria University of Wellington, School of Psychology, Wellington, New Zealand.
JAMA Netw Open. 2020 Dec 1;3(12):e2030898. doi: 10.1001/jamanetworkopen.2020.30898.
It is unclear whether burnout, anxiety, and depression constitute the same or different constructs. Better understanding of these constructs is important for diagnosis and treatment for intensive care unit (ICU) clinicians.
To determine the associations and distinctiveness of burnout, depression, and anxiety in a sample of ICU clinicians.
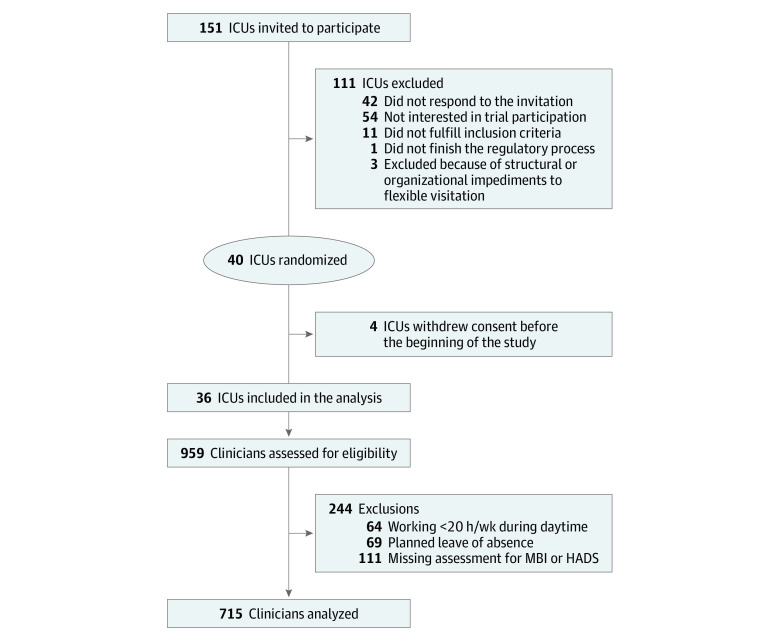
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study used baseline data from the ICU Visits Study, a cluster-randomized crossover clinical trial conducted from April 2017 to July 2018 in 36 mixed public and private nonprofit ICUs in Brazil. ICU clinicians, including day-shift physicians, nurses, nurse technicians, and physiotherapists working in an ICU at least 20 hours per week, were enrolled. Data were analyzed from December 27, 2019, to October 10, 2020.
The main outcome measures were burnout, depression, and anxiety measured with the Maslach Burnout Inventory (MBI; range, 0-6, with high scores indicating more burnout) and the Hospital Depression and Anxiety Scale (HADS; range, 0-3, with higher scores indicating more depression or anxiety). Internal consistencies were satisfactory.
The total sample included 715 ICU clinicians (median [interquartile range] age, 34.8 [30.2-39.3] years; 520 [72.7%] women), including 96 physicians (13.4%), 159 nurses (22.2%), 358 nurse technicians (50.1%), and 102 physiotherapists (14.3%). Clinicians reported low levels of emotional exhaustion (mean [SD] score, 1.84 [1.18]), depersonalization (mean [SD] score, 0.98 [1.03]), and personal accomplishment (mean [SD] score, 5.05 [0.87]) on the MBI, and similarly low levels of depression (mean [SD] score, 0.54 [0.40]) and anxiety (mean [SD] score, 0.70 [0.45]) on the HADS. Confirmatory factor analyses consistently showed improved fit separating latent burnout dimensions from depression and anxiety. An exploratory graph analysis combining gaussian graphical model with clustering algorithms for weighted networks suggested 3 clusters, with distinct burnout, anxiety, and depression clusters. This structure was confirmed using a bootstrap with 1000 random samples, in which the 3-cluster solution emerged in 625 samples (62.5%). Both latent variable loadings and network statistics suggested 3 key indicators (ie, feeling burned out from work, worrying thoughts, and reverse-scored reporting feeling cheerful) that can be used for short screening instruments.
These findings suggest that burnout and clinical symptoms of depression and anxiety were empirically distinct in a large sample of ICU clinicians, highlighting the importance of screening for burnout and clinical symptoms to allow fast access to adequate support and treatment in health professionals at high risk of burnout.
目前尚不清楚倦怠、焦虑和抑郁是否属于同一或不同的结构。更好地理解这些结构对于 ICU 临床医生的诊断和治疗很重要。
确定 ICU 临床医生样本中倦怠、抑郁和焦虑之间的关联和独特性。
设计、地点和参与者:这项横断面研究使用了 ICU 探访研究的基线数据,该研究是一项于 2017 年 4 月至 2018 年 7 月在巴西 36 家混合公立和非营利性 ICU 进行的集群随机交叉临床试验。纳入了每周至少在 ICU 工作 20 小时的日间医生、护士、护士技术员和物理治疗师等 ICU 临床医生。数据分析于 2019 年 12 月 27 日至 2020 年 10 月 10 日进行。
主要结局指标是使用 Maslach 倦怠量表(MBI;范围 0-6,高分表示更多的倦怠)和医院抑郁和焦虑量表(HADS;范围 0-3,更高的分数表示更多的抑郁或焦虑)测量的倦怠、抑郁和焦虑。内部一致性令人满意。
总样本包括 715 名 ICU 临床医生(中位数[四分位数范围]年龄为 34.8[30.2-39.3]岁;520[72.7%]为女性),包括 96 名医生(13.4%)、159 名护士(22.2%)、358 名护士技术员(50.1%)和 102 名物理治疗师(14.3%)。临床医生报告在 MBI 上的情绪耗竭(平均[标准差]评分,1.84[1.18])、去人格化(平均[标准差]评分,0.98[1.03])和个人成就感(平均[标准差]评分,5.05[0.87])水平较低,在 HADS 上的抑郁(平均[标准差]评分,0.54[0.40])和焦虑(平均[标准差]评分,0.70[0.45])水平也较低。验证性因素分析一致表明,将潜在的倦怠维度与抑郁和焦虑分开的拟合度有所提高。一项结合高斯图形模型和加权网络聚类算法的探索性图形分析表明,存在 3 个聚类,具有明显的倦怠、焦虑和抑郁聚类。使用 1000 个随机样本的 bootstrap 方法对其进行了验证,其中 3 聚类解决方案出现在 625 个样本(62.5%)中。潜在变量的负荷和网络统计数据均表明,有 3 个关键指标(即工作倦怠感、担忧思维和反向报告的愉快感)可用于简短的筛查工具。
这些发现表明,在 ICU 临床医生的大样本中,倦怠和临床抑郁及焦虑症状在经验上是不同的,这突出了在有倦怠风险的卫生专业人员中筛查倦怠和临床症状的重要性,以便能够快速获得适当的支持和治疗。
