Kim Kyung Hoon, Jeong Nari, Lim Jeong Uk, Lee Hwa Young, Lee Jongmin, Lee Hye-Yeon, Kim Seok Chan, Kang Ji Young
Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Incheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
Department of Pulmonology, G Sam Hospital, Gunpo, Republic of Korea.
J Thorac Dis. 2022 Apr;14(4):1009-1019. doi: 10.21037/jtd-21-1723.
There have been few studies to verify factors associated with a false-negative interferon-gamma release assay (IGRA) in patients with tuberculous pleurisy. We investigated the clinical relevance of false-negative results of the blood QuantiFERON-TB Gold In-Tube (QFT-GIT) assay and its risk factors in patients diagnosed with pleural tuberculosis (TB).
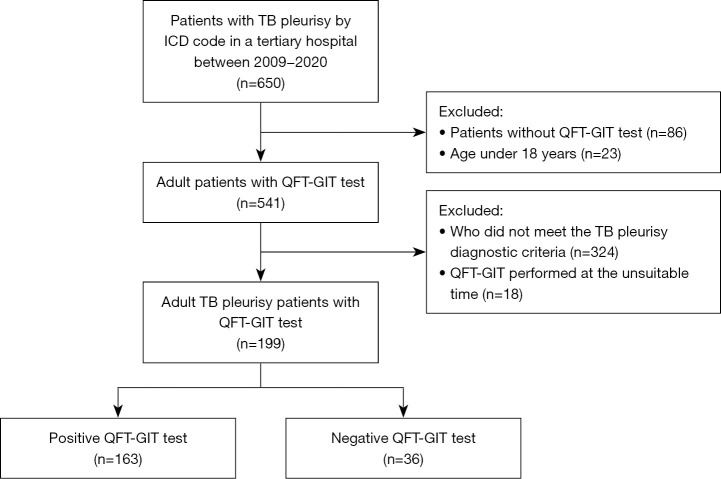
Medical records of 650 pleural TB patients in a tertiary hospital between January 2009 and December 2020 were reviewed retrospectively. Patients who underwent the blood QFT-GIT assay and pleural fluid analysis before starting anti-TB medication were included.
Of 199 patients with pleural TB who were performed QFT-GIT assay, 36 (18.1%) were false-negative results. These patients tended to be older than those with a positive result (P=0.060). The QFT-GIT-false-negative group of had significantly more comorbidities such as end-stage renal disease (ESRD), haematological cancer or pneumoconiosis than the QFT-GIT-positive group. Hypoproteinaemia and pH >6 in pleural fluid were associated with a false-negative QFT-GIT. Of the 199 patients, 163 (81.9%) were cured or completed anti-TB treatment; 13 patients (6.5%) died. The QFT-GIT-negative patients had significantly worse outcomes including mortality [unfavourable outcome: 33.3% (12/36 patients) in QFT-GIT-negative groups 14.7% (24/163 patients) in QFT-GIT-positive groups, P<0.017; overall mortality: 16.7% (6/36 patients) 4.3% (7/163 patients), respectively, P<0.015].
In pleural TB, a false-negative QFT-GIT result was 18.1% in a country of intermediate TB incidence. This discordant result in GFT-GIT was associated with ESRD, pneumoconiosis, hypoproteinaemia and a poor outcome. Clinicians should keep in mind the possibility of false-negativity in the blood IGRA test, especially in specific situations and its impact on TB outcome in managing patients with pleural TB.
很少有研究验证结核性胸膜炎患者中与γ-干扰素释放试验(IGRA)假阴性相关的因素。我们调查了血液结核感染T细胞检测(QFT-GIT)试验假阴性结果在诊断为胸膜结核患者中的临床相关性及其危险因素。
回顾性分析2009年1月至2020年12月期间一家三级医院650例胸膜结核患者的病历。纳入在开始抗结核治疗前接受血液QFT-GIT试验和胸水分析的患者。
在199例接受QFT-GIT试验的胸膜结核患者中,36例(18.1%)为假阴性结果。这些患者往往比结果为阳性的患者年龄更大(P=0.060)。与QFT-GIT阳性组相比,QFT-GIT假阴性组的合并症如终末期肾病(ESRD)、血液系统癌症或尘肺病明显更多。低蛋白血症和胸水pH>6与QFT-GIT假阴性相关。在199例患者中,163例(81.9%)治愈或完成了抗结核治疗;13例(6.5%)死亡。QFT-GIT阴性患者的结局明显更差,包括死亡率[不良结局:QFT-GIT阴性组为33.3%(12/36例患者),QFT-GIT阳性组为14.7%(24/163例患者),P<0.017;总死亡率:分别为16.7%(6/36例患者)和4.3%(7/163例患者),P<0.015]。
在结核发病率中等的国家,胸膜结核患者中QFT-GIT结果假阴性率为18.1%。GFT-GIT中的这种不一致结果与ESRD、尘肺病、低蛋白血症和不良结局相关。临床医生应牢记血液IGRA检测出现假阴性的可能性,尤其是在特定情况下,以及其对胸膜结核患者治疗结局的影响。