Department of Colorectal Surgery, Portsmouth Hospitals NHS Trust, Queen Alexandra Hospital Portsmouth, Portsmouth, UK.
University of Portsmouth, Portsmouth, UK.
Surg Endosc. 2021 Dec;35(12):6873-6881. doi: 10.1007/s00464-020-08194-z. Epub 2021 Jan 5.
Complete mesocolic excision (CME) for right colon cancers has traditionally been an open procedure. Surgical adoption of minimal access CME remains limited due to the technical challenges, training gaps and lack of level-1 data for proven benefits. Currently there is limited published data regarding the clinical results with the use of robotic CME surgery. Aim To report our experience, results and techniques, highlighting a clinical and oncological results and midterm oncological outcomes for robotic CME.
To report our experience, results and techniques, highlighting a clinical and oncological results and midterm oncological outcomes for robotic CME.
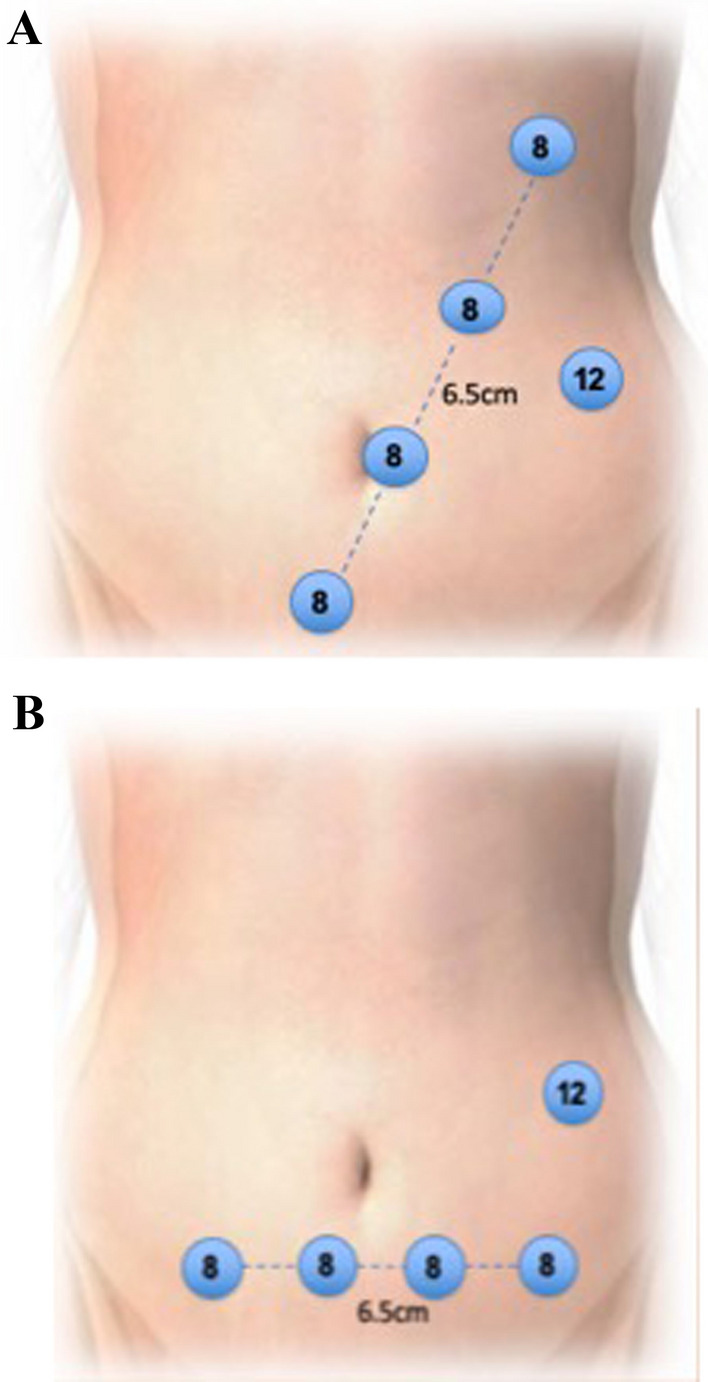
All patients undergoing standardised robotic CME technique with SMV first approach between January 2015 and September 2019 were included in this retrospective review of a prospectively collected database. Patient demographics, operative data and clinical and oncological outcomes were recorded.
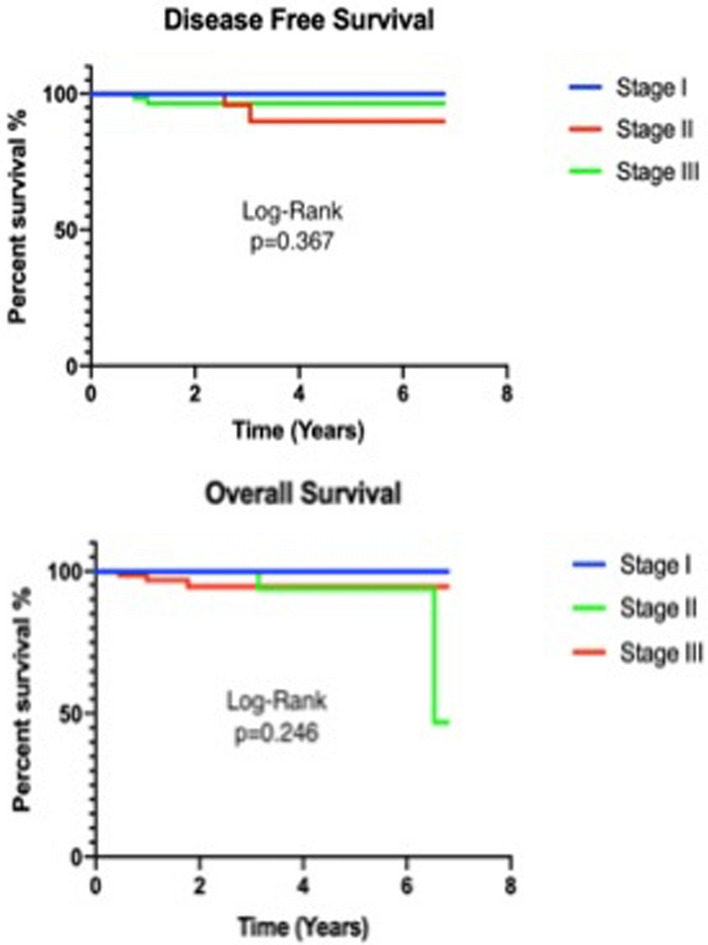
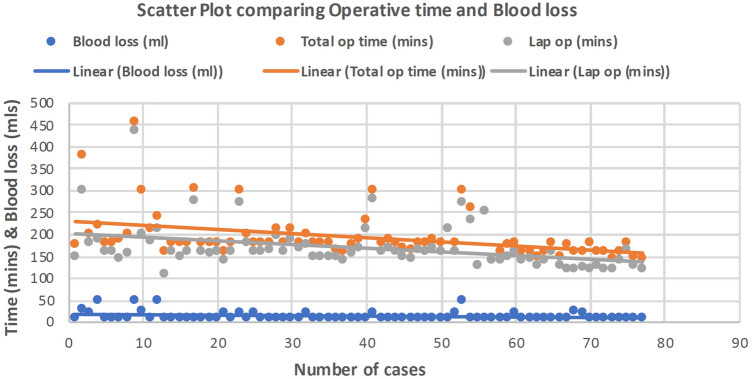
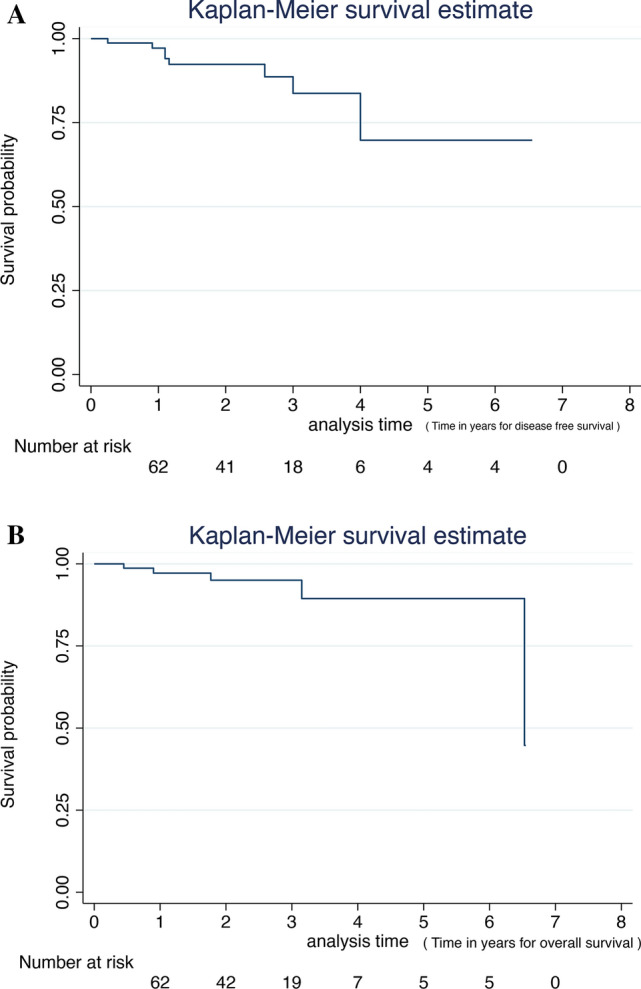
Seventy-seven robotic CME resections for right colonic cancers were performed over a 4-year period. Median operative time was 180 (128-454) min and perioperative blood loss was 10 (10-50) ml. There were 25 patients who had previous abdominal surgery. Median postoperative hospital stay was 5 (3-18) days. There was no conversion to open surgery in this series. Median lymph node count was 30 (10-60). Three (4%) patients had R1 resection. There was one (1%) local recurrence in stage III disease and 4(5%) distal recurrence in stage II and stage III. There was no 30- or 90-day mortality. Three-year disease-free survival was 100%, 91.7% and 92% for stages I, II and III, respectively. Overall survival was 94%.
Robotic CME is feasible, effective and safe. Good oncological results and improved survival are seen in this cohort of patients with a standardised approach to robotic CME.
传统上,右半结肠癌的完整结肠系膜切除术(CME)是一种开放性手术。由于技术挑战、培训差距以及缺乏经过验证的获益水平 1 数据,微创 CME 的手术应用仍然有限。目前,关于使用机器人 CME 手术的临床结果的相关数据有限。目的:报告我们的经验、结果和技术,重点介绍机器人 CME 的临床和肿瘤学结果以及中期肿瘤学结果。
报告我们的经验、结果和技术,重点介绍机器人 CME 的临床和肿瘤学结果以及中期肿瘤学结果。
本回顾性研究纳入了 2015 年 1 月至 2019 年 9 月期间接受标准化机器人 CME 技术(SMV 先行法)的所有患者。记录患者的人口统计学数据、手术数据以及临床和肿瘤学结果。
在 4 年的时间里,共进行了 77 例右半结肠癌的机器人 CME 切除术。中位手术时间为 180 分钟(128-454 分钟),围手术期出血量为 10 毫升(10-50 毫升)。有 25 例患者曾接受过腹部手术。中位术后住院时间为 5 天(3-18 天)。在本系列中,无中转开放手术。中位淋巴结计数为 30 枚(10-60 枚)。3 例(4%)患者行 R1 切除术。在 III 期疾病中,有 1 例(1%)局部复发,在 II 期和 III 期疾病中,有 4 例(5%)远端复发。无 30 天或 90 天死亡率。I、II 和 III 期患者的 3 年无病生存率分别为 100%、91.7%和 92%。总生存率为 94%。
机器人 CME 是可行的、有效的且安全的。在本队列中,采用标准化的机器人 CME 方法可获得良好的肿瘤学结果和更高的生存率。