Centre for Global Child Health, Hospital for Sick Children, 555 University avenue, Toronto, ON, M5G 1X8, Canada.
Social System Design Lab, Brown School of Social Work and Public Health, Washington University in St Louis, St-Louis, MO, USA.
BMC Health Serv Res. 2021 Jan 6;21(1):26. doi: 10.1186/s12913-020-06014-7.
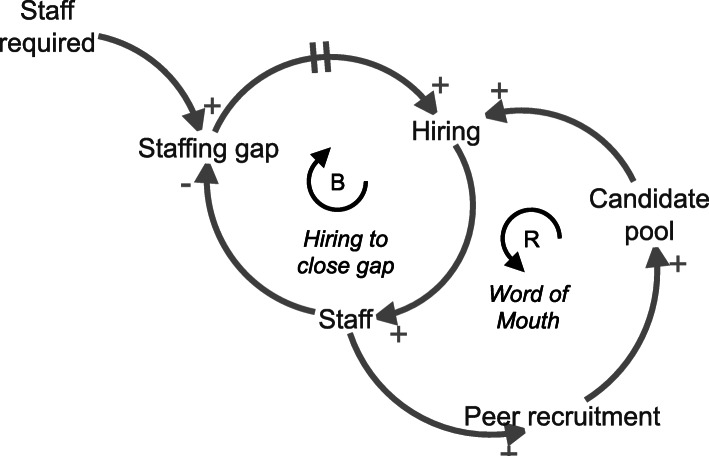
Group model building (GMB) is a method to facilitate shared understanding of structures and relationships that determine system behaviors. This project aimed to determine the feasibility of GMB in a resource-limited setting and to use GMB to describe key barriers and facilitators to effective acute care delivery at a tertiary care hospital in Malawi.
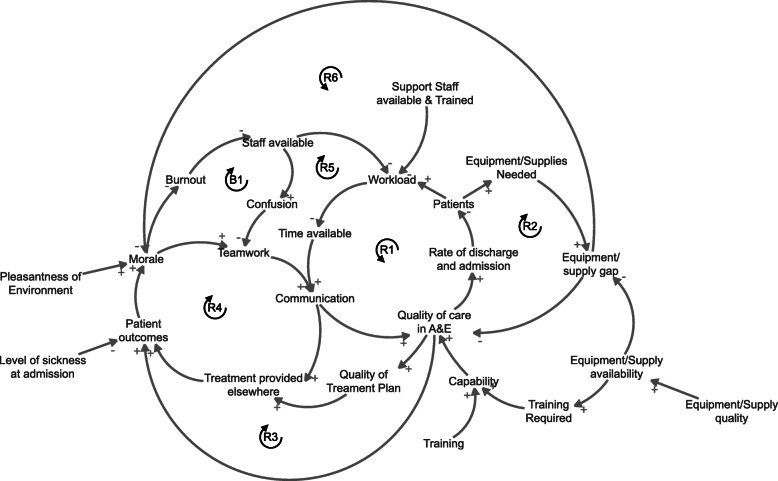
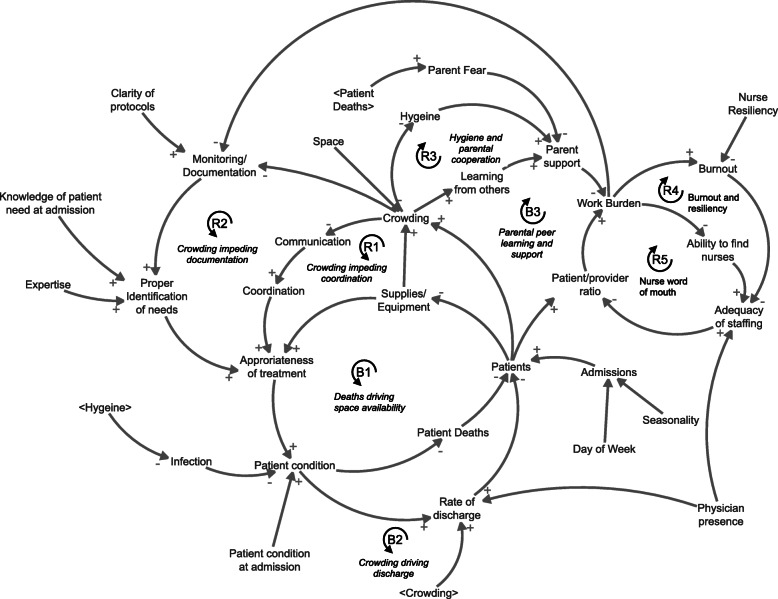
Over 1 week, trained facilitators led three GMB sessions with two groups of healthcare providers to facilitate shared understanding of structures and relationships that determine system behaviors. One group aimed to identify factors that impact patient flow in the paediatric special care ward. The other aimed to identify factors impacting delivery of high-quality care in the paediatric accident and emergency room. Synthesized causal maps of factors influencing patient care were generated, revised, and qualitatively analyzed.
Causal maps identified patient condition as the central modifier of acute care delivery. Severe illness and high volume of patients were identified as creating system strain in several domains: (1) physical space, (2) resource needs and utilization, (3) staff capabilities and (4) quality improvement. Stress in these domains results in worsening patient condition and perpetuating negative reinforcing feedback loops. Balancing factors inherent to the current system included (1) parental engagement, (2) provider resilience, (3) ease of communication and (4) patient death. Perceived strengths of the GMB process were representation of diverse stakeholder viewpoints and complex system synthesis in a visual causal pathway, the process inclusivity, development of shared understanding, new idea generation and momentum building. Challenges identified included time required for completion and potential for participant selection bias.
GMB facilitated creation of a shared mental model, as a first step in optimizing acute care delivery in a paediatric facility in this resource-limited setting.
群体模式构建(GMB)是一种促进对决定系统行为的结构和关系的共同理解的方法。本项目旨在确定在资源有限的环境中 GMB 的可行性,并使用 GMB 描述马拉维一家三级保健医院有效提供急性护理服务的主要障碍和促进因素。
在一周的时间里,经过培训的协调员与两组医疗服务提供者一起进行了三次 GMB 会议,以促进对决定系统行为的结构和关系的共同理解。一组旨在确定影响儿科特殊护理病房患者流动的因素。另一组旨在确定影响儿科急诊室高质量护理提供的因素。生成、修订和定性分析了影响患者护理的因素综合因果图。
因果图确定患者状况是急性护理提供的核心调节因素。严重疾病和大量患者被确定为在几个领域造成系统紧张:(1)物理空间,(2)资源需求和利用,(3)员工能力和(4)质量改进。这些领域的压力导致患者病情恶化,并使负面的增强反馈循环持续存在。当前系统中固有的平衡因素包括(1)父母参与,(2)提供者韧性,(3)沟通便利性和(4)患者死亡。GMB 过程的感知优势包括代表不同利益相关者的观点和在视觉因果途径中对复杂系统的综合、包容性的过程、共同理解的发展、新想法的产生和动力的建立。确定的挑战包括完成所需的时间和参与者选择偏差的潜在风险。
GMB 促进了在资源有限的环境中建立一个儿科设施中急性护理提供的共同心理模型,这是优化急性护理提供的第一步。