Miller Andrew C, Scissum Kiyoshi, McConnell Lorena, East Nathaniel, Vahedian-Azimi Amir, Sewell Kerry A, Zehtabchi Shahriar
Department of Emergency Medicine, Nazareth Hospital, Philadelphia College of Osteopathic Medicine, Philadelphia, PA, USA.
Department of Emergency Medicine, East Carolina University, Greenville, NC, USA.
Int J Crit Illn Inj Sci. 2020 Jul-Sep;10(3):109-122. doi: 10.4103/IJCIIS.IJCIIS_155_20. Epub 2020 Sep 22.
Restoring cardiopulmonary circulation with effective chest compression remains the cornerstone of resuscitation, yet real-time compressions may be suboptimal. This project aims to determine whether in patients with in-hospital cardiac arrest (IHCA; population), chest compressions performed with free-standing audiovisual feedback (AVF) device as compared to standard manual chest compression (comparison) results in improved outcomes, including the sustained return of spontaneous circulation (ROSC), and survival to the intensive care unit (ICU) and hospital discharge (outcomes).
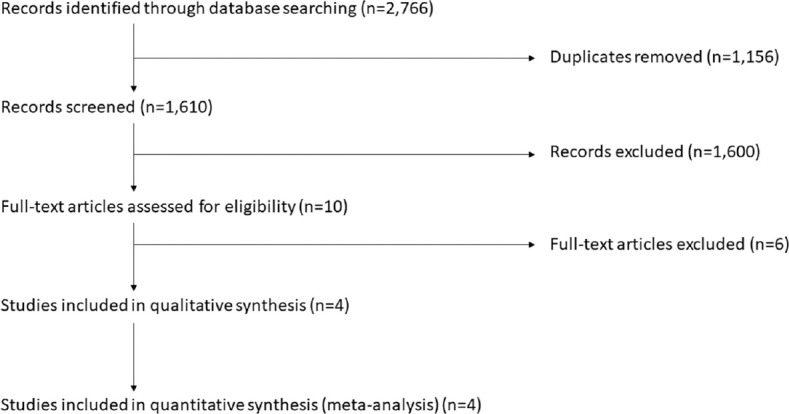
Scholarly databases and relevant bibliographies were searched, as were clinical trial registries and relevant conference proceedings to limit publication bias. Studies were not limited by date, language, or publication status. Clinical randomized controlled trials (RCT) were included that enrolled adults (age ≥ 18 years) with IHCA and assessed real-time chest compressions delivered with either the standard manual technique or with AVF from a freestanding device not linked to an automated external defibrillator (AED) or automated compressor.
Four clinical trials met inclusion criteria and were included. No ongoing trials were identified. One RCT assessed the Ambu CardioPump (Ambu Inc., Columbia, MD, USA), whereas three assessed Cardio First Angel™ (Inotech, Nubberg, Germany). No clinical RCTs compared AVF devices head-to-head. Three RCTs were multi-center. Sustained ROSC (4 studies, = 1064) was improved with AVF use (Relative risk [RR] 1.68, 95% confidence interval [CI] 1.39-2.04), as was survival to hospital discharge (2 studies, = 922; RR 1.78, 95% CI 1.54-2.06) and survival to hospital discharge (3 studies, = 984; RR 1.91, 95% CI 1.62-2.25).
The moderate-quality evidence suggests that chest compressions performed using a non-AED free-standing AVF device during resuscitation for IHCA improves sustained ROSC and survival to ICU and hospital discharge.
PROSPERO (CRD42020157536).
通过有效的胸外按压恢复心肺循环仍然是复苏的基石,但实时按压可能并非最佳。本项目旨在确定在院内心脏骤停(IHCA;人群)患者中,与标准手动胸外按压(对照)相比,使用独立视听反馈(AVF)设备进行胸外按压是否能改善预后,包括自主循环恢复(ROSC)的持续恢复、重症监护病房(ICU)存活及出院(预后)。
检索学术数据库和相关参考文献,以及临床试验注册库和相关会议论文集以限制发表偏倚。研究不受日期、语言或发表状态限制。纳入的临床随机对照试验(RCT)为成年(年龄≥18岁)IHCA患者,评估采用标准手动技术或来自未与自动体外除颤器(AED)或自动压缩机相连的独立设备的AVF进行的实时胸外按压。
四项临床试验符合纳入标准并被纳入。未识别出正在进行的试验。一项RCT评估了美国马里兰州哥伦比亚市Ambu公司的Ambu CardioPump,而三项评估了德国纽伯格Inotech公司的Cardio First Angel™。没有临床RCT对AVF设备进行直接比较。三项RCT为多中心试验。使用AVF可改善持续ROSC(4项研究, = 1064;相对风险[RR] 1.68,95%置信区间[CI] 1.39 - 2.04),出院存活率(2项研究, = 922;RR 1.78,95% CI 1.54 - 2.06)以及存活至出院(3项研究, = 984;RR 1.91,95% CI 1.62 - 2.25)。
中等质量证据表明,在IHCA复苏期间使用非AED独立AVF设备进行胸外按压可改善持续ROSC以及ICU存活和出院存活率。
PROSPERO(CRD42020157536)